


Application and interpretation of non-invasive testing in MetALD
 0
0 
Abstract
Metabolic dysfunction and alcohol-related liver disease (MetALD) is a newly defined entity describing individuals with metabolic dysfunction-associated steatotic liver disease (MASLD) and increased alcohol intake, but below the threshold for a primary diagnosis of alcohol-related liver disease (ALD). This narrative review provides a state-of-the-art overview of the clinical application and interpretation of non-invasive tests (NITs) in MetALD. Due to a current paucity of disease-specific data, we evaluate NITs for steatosis, inflammation, fibrosis, and prognostication for MetALD by drawing upon established MASLD research. We further examine methods for evaluating alcohol intake, ranging from comprehensive clinical histories and screening tools to dedicated biomarkers. While MASLD-derived NITs appear applicable to MetALD, episodic binge drinking can confound results. Therefore, accuracy may be improved by incorporating validated binge assessments and ensuring a minimum alcohol-free interval before testing. Finally, this review addresses the role of NITs in clinical trials for MetALD. For years, the histological response of metabolic dysfunction-associated steatohepatitis (MASH) resolution and fibrosis improvement has been the only reasonably likely surrogate endpoint used for accelerated drug approval. Consequently, thousands of patients have undergone invasive repeated liver biopsies, highlighting the need for validated noninvasive alternatives in future drug development. As the regulatory pathway for MetALD drug development is still evolving, there is a critical opportunity to engage stakeholders and implement NIT-based trial designs to improve patient safety and accelerate therapeutic advancement.
Keywords
INTRODUCTION
Recent nomenclature changes replaced non-alcoholic fatty liver disease with metabolic dysfunction-associated steatotic liver disease (MASLD). This term defines hepatic steatosis occurring with at least one cardiometabolic risk factor (CMRF). Concurrently, a new entity called metabolic dysfunction and alcohol-related liver disease (MetALD) was introduced to describe patients with MASLD and increased alcohol intake (20-50 g/day for women; 30-60 g/day for men). Individuals exceeding these intake thresholds are classified as having alcohol-related liver disease (ALD)[1]. The shift to MASLD more clearly attributes the condition to its underlying metabolic etiology. This clarity has successfully heightened awareness beyond hepatology, exemplified by the American Diabetes Association’s dedicated consensus report[2]. Furthermore, these changes align with broader advancements in metabolic medicine. This includes the clinical recognition of obesity as a condition related to excess adiposity, organ dysfunction, and functional limitations[3]. Within hepatology, recent milestones include the conditional approval of two pharmacological therapies for metabolic dysfunction-associated steatohepatitis (MASH)[4,5], with several others in development. Non-invasive tests (NITs) have also advanced significantly, improving diagnosis, prognostication, patient selection for treatment, and treatment monitoring[6]. Amidst these MASLD-focused developments, MetALD has emerged as a distinct area of interest. Research into its epidemiology, assessment, and management is expanding rapidly. This narrative review evaluates the application and interpretation of NITs in MetALD, drawing on MASLD-derived insights while treating MetALD as a unique clinical entity.
EVALUATION OF STEATOSIS, INFLAMMATION AND FIBROSIS IN METALD
MASLD and ALD share common pathophysiological pathways in terms of liver injury and fibrosis. While MASLD is primarily driven by insulin resistance and lipotoxicity from chronic nutritional excess, ALD results from alcohol and its toxic metabolite, acetaldehyde[7]. Histologically, they share similar features, although certain changes are more commonly seen in alcohol-related liver injury but are rare or not well-described in MASLD[8]. Consequently, diagnostic tools for evaluating both conditions are largely analogous. As a hybrid entity, MetALD likely attenuates these differences, though specific data remain limited due to its recent introduction. The following sections review the current landscape of NITs in MASLD, followed by an examination of emerging studies that validate these tools in MetALD cohorts while addressing evidentiary gaps through research in ALD.
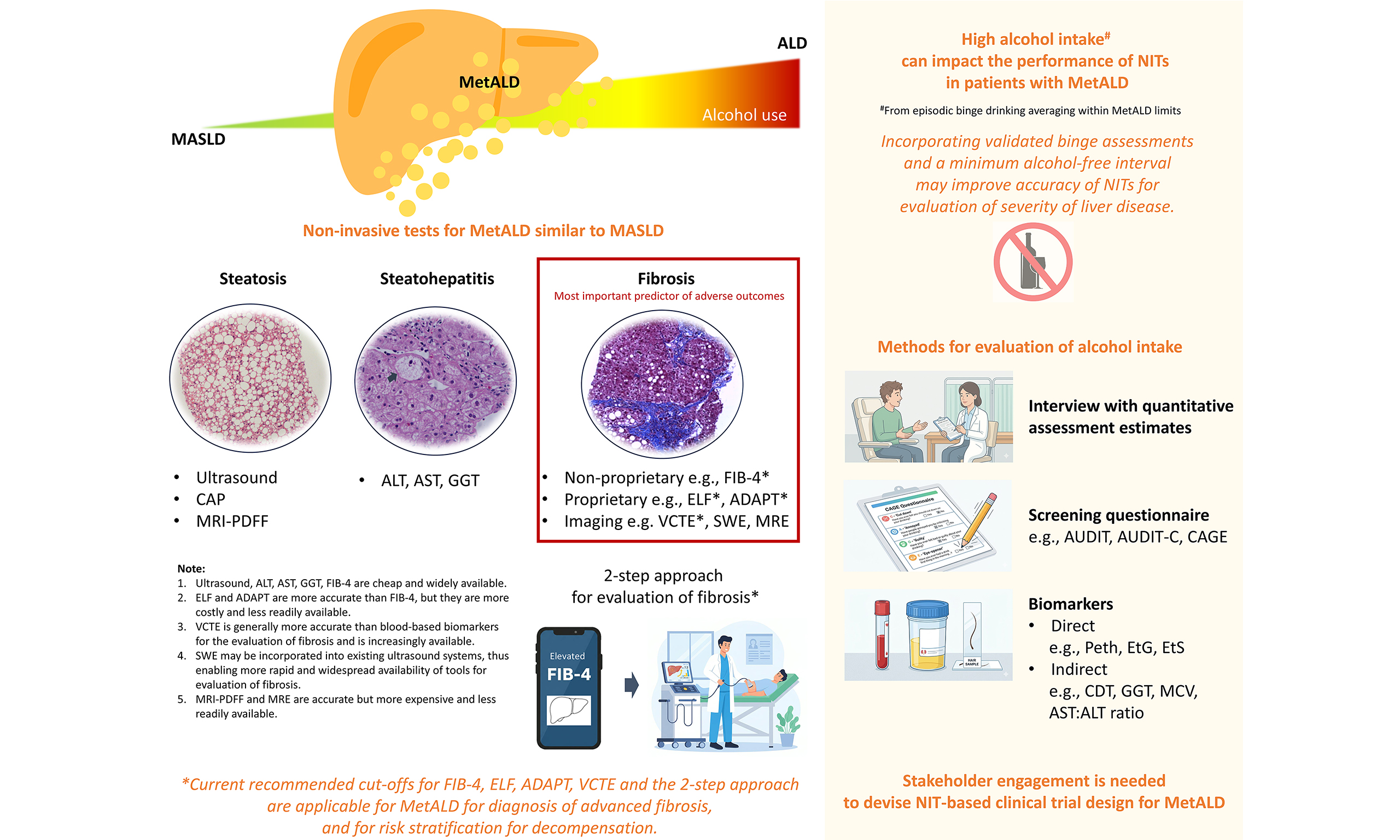
Hepatic steatosis is commonly diagnosed via ultrasonography, which offers up to 92% sensitivity for moderate-to-severe cases but often misses mild involvement[9]. Controlled attenuation parameter (CAP) allows for simultaneous steatosis assessment during liver stiffness measurement (LSM) using vibration-controlled transient elastography (VCTE)[6]. While magnetic resonance imaging proton density fat fraction (MRI-PDFF) provides highly accurate quantification, its use remains largely restricted to research settings[10]. To evaluate necro-inflammation, serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are standard; however, levels may remain normal even during active injury or advanced disease[11]. Alcohol-related liver injury typically results in more pronounced elevations of AST and gamma-glutamyl transferase (GGT) due to the direct effects of alcohol[12].
Fibrosis remains the most critical predictor of adverse liver-related outcomes[13]. Assessment tools include blood-based biomarkers and imaging techniques[14]. Among non-proprietary blood-based biomarkers, the Fibrosis-4 (FIB-4) index is widely used due to its low cost and high negative predictive value in MASLD populations[6]. Proprietary options include the Enhanced Liver Fibrosis (ELF) panel[15]. Imaging-based techniques include VCTE, shear wave elastography (SWE), and magnetic resonance elastography (MRE)[16]. VCTE is the most studied imaging-based technique for evaluation of fibrosis, including the development of novel scores such as the Fibroscan-AST (FAST) score[17], Agile 3+ and Agile 4 score[18]. Interest in SWE is growing as it can be integrated into standard ultrasound systems, potentially increasing availability[19]. MRE, though accurate, is limited by high costs and the need for dedicated hardware.
The high prevalence of MASLD, its asymptomatic progression, and the small subset of patients with severe liver disease present significant clinical challenges. Consequently, major guidelines now advocate for a two-step approach to identify patients with more severe liver disease: screening with FIB-4 followed by LSM for those with elevated scores[20,21]. Furthermore, the field is shifting from biopsy toward NIT-based risk stratification. The concept of compensated advanced chronic liver disease (cACLD) stratifies the risks of clinically significant portal hypertension and decompensation in people with chronic liver disease based on LSM, regardless of histological stage and the ability of LSM to identify these stages[22].
Further studies would increase our certainty on the applicability and interpretation of the aforementioned NITs and approaches in MetALD. Several such recent and noteworthy works are summarized in Table 1[23-25]. Another review article approached NITs for MetALD from a different perspective, focusing through the lens of ALD[26]. There will be specific nuances that need to be considered when using NITs in day-to-day clinical practice. Emerging evidence suggests that alcohol intake can dynamically alter liver fat and stiffness; for instance, binge drinking can temporarily increase both, with resolution after abstinence[27]. In individuals with heavy alcohol use or episodic binge drinking, elevated serum aminotransferase levels and reduced platelet counts - resulting from alcohol's direct toxic effects - often confound the FIB-4 index. These biochemical alterations potentially compromise the tool's diagnostic accuracy for fibrosis staging. Furthermore, alcohol-induced necro-inflammation can elevate LSM, leading to overestimations of fibrosis severity. Evidence suggests that delaying LSM until serum AST levels fall below 100 IU/L following a period of abstinence significantly improves diagnostic accuracy for cirrhosis[28]. Because the current MetALD definition relies on average alcohol intake rather than drinking patterns, episodic binge drinkers may be classified as MetALD patients despite having intake levels that impair the performance of NITs. Incorporating validated binge assessments (see section on Evaluation of alcohol intake in MetALD) and a mandatory alcohol-free interval may refine the accuracy of NITs in assessing liver disease severity. Alternatively, recalibrating MASLD-derived NIT cutoffs could preserve specificity against alcohol-related inflammation. However, this approach remains limited by inter-individual variability in biomarker response and the increased complexity of clinical implementation.
Studies on non-invasive tests in MetALD
| Author, year | Study population | Main findings |
| Oh et al., 2024[23] | Health check participants who underwent MRE, 462 had MetALD, 2,652 had MASLD | The AUROC for FIB-4 for diagnosis of advanced fibrosis (based on MRE ≥ 3.6 kPa) was similar between MetALD and MASLD (0.85 vs. 0.80) with similar sensitivity (71.4% vs. 68.2%), specificity (77.3% vs. 75.8%), PPV (4.6% vs. 6.4%) and NPV (99.4% vs. 98.9%, p not significant for all comparisons) |
| Torp et al., 2025[25] | 423 patients with steatotic liver disease, 24% had MetALD | The AUROC (95%CI) for FIB-4 for diagnosis of advanced fibrosis (based on histology) was similar between MetALD [0.80 (0.69-0.91)] and MASLD [0.80 (0.74-0.86)]. ELF [0.90 (0.83-0.97)] and ADAPT [0.90 (0.81-0.98)] had highest AUROC for diagnosis of advanced fibrosis in MetALD; similar in MASLD [0.86 (0.81-0.92) and 0.83 (0.77-0.90)]. Current recommended cut-offs for FIB-4, ELF and ADAPT are applicable for MetALD for diagnosis of advanced fibrosis, and for risk stratification for decompensation, including VCTE and the 2-step approach* |
| Diaz et al., 2025[24] | 97 individuals with suspected MetALD based on self-reported alcohol use or PEth testing, 8% significant fibrosis | The AUROC (95%CI) for FIB-4 (using ≥ 1.3 cut-off) for diagnosis of significant fibrosis (based on MRE ≥ 3.14 kPa or VCTE ≥ 7.6 kPa if MRE was missing) was 0.78 (0.58-0.98) with sensitivity 80%, specificity 76%, PPV 17% and NPV 98%. For VCTE (using ≥ 8 kPa cut-off, the corresponding values are 0.85 (0.66-1.00), 80%, 91%, 36% and 99%, respectively. Using the 2-step approach*, the false negative rate of individuals classified as low risk who truly have significant fibrosis was 2% of the entire cohort |
PROGNOSTIC SCORES FOR METALD
As MetALD is a relatively new construct defined in 2023[29], disease-specific prognostic scores and long-term natural history studies remain limited. Most current research has focused on validating existing non-invasive scores originally developed for other chronic liver diseases. Interpreting these results requires an understanding of how the MetALD prognosis differs from MASLD and ALD. MetALD involves two synergistic drivers of progression: alcohol consumption and CMRFs[29]. Both increased alcohol intake - measured via self-report or phosphatidylethanol (PEth) - and a higher number of CMRFs independently correlate with increased liver-related events and all-cause mortality in MASLD patients[30,31]. While the individual contribution of each factor is still being researched[8], recent UK Biobank data suggest that “alcohol-predominant” MetALD carries a poorer prognosis than “cardiometabolic-predominant” phenotypes[32]. Indeed, it is well-established that ALD has faster disease progression and a worse prognosis compared with MASLD[30,33]. Taken together, it is expected that the prognosis of MetALD (where the alcohol exposure is less than that of ALD) would be between that of MASLD and ALD. Consistent with this, large meta-analyses and population-based studies report higher rates of liver-related events in MetALD than MASLD, with mixed data for all-cause mortality, while ALD cohorts repeatedly demonstrate worse outcomes compared to both MASLD and MetALD[32,34-38].
With an estimated prevalence of 2%-8%, MetALD affects a substantial portion of the population[26]. Similar to other chronic liver diseases, its management and triage depend on the extent of fibrosis[39]. Established NITs, such as FIB-4 and LSM, have recently been validated in MetALD cohorts across South Korea, Denmark, and the United States. These scores consistently show strong performance in predicting advanced fibrosis and clinical outcomes [area under the receiver operating characteristic curve (AUROC) or C-statistics > 0.75], utilizing the same cut-offs as other liver diseases [Table 2]. Similar to MASLD, applying a stepwise algorithm using two or three NITs reduces the number of patients with indeterminate results and unnecessary referrals to secondary care[24,25]. For example, in a study to detect MRE-defined significant fibrosis in patients with MetALD, performing LSM in patients with indeterminate FIB-4 resulted in overall indeterminate results in 1% only with a very low false negative rate of 2%[24].
Non-invasive tests validated in MetALD patients focusing on individual tests and their diagnostic performance and suggested cut-offs
| Test name | Variables in test | Validation and performance in MetALD | Suggested cut-off in MetALD |
| FIB-4 index[23-25] | Age, ALT, AST, platelet count | AUROC - 0.85 for detecting advanced fibrosis* - 0.78 for detecting significant fibrosis# Harrel’s C-statistic - 0.82 for predicting decompensation and death | < 1.3 = low risk 1.3-2.67 = indeterminate > 2.67 = high risk |
| NFS[23] | Age, BMI, glucose status, AST/ALT ratio, platelet count, albumin | AUROC - 0.85 for detecting advanced fibrosis* | Not reported |
| SAFE score[38] | Age, BMI, diabetes, ALT, AST, globulin, platelet count | Stratified MetALD patients into low, intermediate and high risk for all-cause death (univariable model) | < 0 = low risk 0- < 100 = intermediate risk ≥ 100 = high risk |
| ELF score[25] | Hyaluronic Acid, PIIINP, TIMP-1 | Harrel’s C-statistic - 0.78 for predicting decompensation and death | < 9.8 = low risk 9.8-11.3 = indeterminate > 11.3 = high risk |
| ADAPT score[25] | Age, diabetes, PRO-C3, platelet count | Harrel’s C-statistic - 0.80 for predicting decompensation and death | < 6.33 = low risk 6.33-7.15 = indeterminate > 7.15 = high risk |
| LiverRisk score[25] | Age, sex, fasting glucose, cholesterol, ALT, AST, GGT, platelet count | Harrel’s C-statistic - 0.77 for predicting decompensation and death | < 10 = low risk 10- < 15 = medium risk ≥ 15 = high risk |
| Vibration controlled transient elastography[24,25] | Liver stiffness measurement | AUROC - 0.85 for detecting significant fibrosis# Harrel’s C-statistic - 0.78 for predicting decompensation and death | For significant fibrosis: < 8 kPa = low risk 8-12 kPa = indeterminate ≥ 12 kPa = high risk For decompensations and death: < 10 kPa = low risk 10-15 kPa = indeterminate ≥ 15 kPa = high risk |
| Liu et al.’s concise 10-protein model[32] | MAMDC4, SSC4D, CEACAM16, CHI3L1, GGT1, C4BPB, CDHR5, OXT, FCAMR and ADAM22 | “Alcohol-predominant” subgroup had higher fibrosis, incident cirrhosis and mortality than “cardiometabolic-predominant” subgroup | Not reported |
Therefore, the current application of prognostic scores in MetALD is similar to that in MASLD and ALD: to stratify patients according to their risk of adverse clinical outcomes so that appropriate interventions can be implemented to mitigate these outcomes. However, these scoring systems fail to account for the synergistic prognostic impact of continued alcohol exposure and CMRFs that fundamentally characterize the MetALD phenotype. In the future, MetALD-specific prognostic scores incorporating PEth and/or CMRFs may improve discrimination over existing scores, albeit at the cost of the simplicity and versatility of etiology-independent scores that already perform well in MetALD. To date, only one MetALD-specific prognostic model has been developed (mentioned above) using proteome data from ten proteins which can differentiate MASLD from ALD with an AUROC of 0.93[32]. Using this same model to stratify MetALD patients, the authors identified “alcohol-predominant” and “cardiometabolic-predominant” phenotypes; the former exhibited significantly higher FIB-4 scores, as well as increased rates of incident cirrhosis and all-cause mortality. Such scores may help identify patients who require more intensive medical intervention, as well as guide the prioritization of interventions (e.g., targeting excessive alcohol consumption vs. optimizing CMRFs). For example, in patients with low alcohol exposure but high cardiometabolic risk, management should focus on cardiovascular risk reduction. By contrast, in patients with low cardiovascular risk but high alcohol consumption, management should focus on interventions to reduce or stop alcohol intake because of its association with liver disease, cardiovascular disease, and cancer. Clearly, improving and personalizing prognostication in MetALD will remain an area of ongoing research.
Although not specifically studied in MetALD, traditional prognostic scores such as Child-Pugh and the model for end-stage liver disease (MELD) remain applicable once MetALD progresses to established cirrhosis, as they capture downstream consequences of portal hypertension and hepatic synthetic dysfunction that are largely etiology agnostic.
EVALUATION OF ALCOHOL INTAKE IN METALD
Under the new steatotic liver disease framework, quantifying alcohol intake is the critical factor for distinguishing between MASLD, MetALD, and ALD[1]. However, accurate assessment is often hindered by social stigma, cultural factors[40], and subconscious underestimation[41]. Such misclassification can lead to missed treatment opportunities, suboptimal care, and worsened clinical outcomes[42,43].
A comprehensive history - covering recent and lifetime intake, drinking patterns, and duration - remains the primary assessment tool[8]. Clinicians should supplement patient self-reports with collateral information from family or medical records. Because standard drink sizes and alcohol percentages vary globally[44], all intake must be converted into standardized units (grams per day or week) for objective classification[8]. Several psychometric instruments using validated structured questionnaires to evaluate alcohol consumption are available. The Alcohol Use Identification Test (AUDIT), developed by the World Health Organization, utilizes a ten-question survey to screen for alcohol problems, with a score of 8 or higher considered a positive screen for alcohol use disorder[45]. The Alcohol Use Identification Test Consumption (AUDIT-C) instrument is an abbreviated version of AUDIT, focusing on the first three questions in AUDIT that are useful as an initial screen for at-risk drinking patterns. A score of 3 or more in women and 4 or more in men signifies a positive result[46]. The CAGE questionnaire is another instrument used for screening, with further investigation recommended for a score of 2 or more[47]. Other approaches such as lifetime drinking history and timeline follow-back instruments may also be utilized to provide quantitative estimates of alcohol consumption[8].
Direct and indirect biomarkers may further complement the clinical assessment of alcohol consumption, providing objective validation of self-reported intake[8]. Direct markers are metabolite products of alcohol and include ethyl glucuronide (EtG), ethyl sulfate, fatty acid ethyl esters and PEth. Indirect markers reflect physiologic effects of chronic alcohol consumption and can be alcohol specific, such as carbohydrate-deficient transferrin (CDT), or non-specific, such as GGT, mean corpuscular volume (MCV) or AST to ALT ratio[41].
Of note, PEth, an abnormal phospholipid formed in response to presence of alcohol in the body, has emerged as one of the most promising biomarkers for alcohol assessment. This blood-based test is both sensitive and specific, directly correlating with recent and chronic alcohol consumption up to a 4-week detection window[41]. Current consensus suggests a PEth range of 20-200 ng/mL aligns with the 140-420 g weekly alcohol limit that defines MetALD[8]. Increasingly, PEth testing has been performed to monitor alcohol use in context of liver transplantation[48]. PEth testing has also demonstrated clinical utility as an objective quantitative alcohol biomarker that can aid identification of MetALD and ALD subcategories alongside clinical history while reducing diagnostic misclassification[49]. At present, PEth testing remain limited by cost and accessibility constraints, and is suggested to be interpreted in combination with other aspects of assessment and clinical context[8].
Overall, a corroborative framework comprising various permutations of detailed history-taking, self-reporting, adjunct screening tools and dedicated alcohol biomarkers (summarized in Table 3) would enable better triangulation of accurate assessment of alcohol consumption[41]. Biomarkers have the potential to be incorporated into various interpretation framework, for example (1) as an objective covariate (compared with self-reporting) to adjust for the confounding effects of alcohol; (2) as a stratification tool for subgroup analysis whereby specific biomarker thresholds can be used to categorize individuals into different groups with various levels of alcohol use; and (3) as a parallel endpoint to validate self-reported alcohol use, especially in clinical trials looking at alcohol-use disorder or MetALD where alcohol use should at least be one of the secondary endpoints.
Modalities of alcohol consumption evaluation
| Assessment modality | Instrument | Profile |
| Screening questionnaire | AUDIT[45] | 10 item survey about alcohol consumption, symptoms and consequences of drinking; scale 0-40, score > 8 suggest AUD |
| AUDIT-C[46] | 3 item survey to screen for risky drinking pattern; scale 0-12, score > 4 in men and > 3 in women is positive | |
| CAGE questionnaire[47] | Brief 4 question survey to screen for alcohol related problems; scale 0-4, score > 2 warrants further evaluation | |
| Interview with quantitative assessment estimates[8] | Lifetime drinking history | Retrospective interview inquiring about alcohol use from onset of regular drinking to current pattern |
| Timeline follow-back | Reference standard for accurately assessing alcohol consumption within a pre-defined time frame, e.g., weeks to months using calendar | |
| Biomarker[41] | ||
| Direct | PEth | Blood-based marker to assess chronic alcohol consumption, detection window 2-4 weeks, sensitivity 96%-100%, specificity 73%-97% |
| EtG | Urine or hair-based marker to assess recent alcohol intake within 3-day window (urine) sensitivity 71%-89% specificity 92%-99% or longer window 3-6 months (hair) sensitivity 84%-100%, specificity 88%-100% | |
| EtS | Urine-based marker, detection window 3-7 days, sensitivity 86%-89%, specificity 73%-82% | |
| Indirect | CDT | Blood-based marker, detection window 4 weeks, sensitivity 21%-30%, specificity 96%-100% |
| GGT | Non-specific surrogate that is elevated with excessive alcohol intake; it can be raised due to many other factors | |
| MCV | Increased MCV may be related to chronic alcohol intake, non-specific | |
| AST to ALT ratio | Increased AST:ALT ratio may suggest alcohol related liver disease, non-specific | |
CLINICAL TRIAL ENDPOINTS
No clinical trials have been completed specifically for the MetALD population, but parallels can be drawn from MASH drug development. Currently, the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) require histological evidence - MASH resolution and fibrosis improvement - via paired liver biopsies for accelerated approval. Since histological response is, after all, just another surrogate endpoint, full drug approval will be granted after a drug is shown to prevent “hard” clinical endpoints, including progression to cirrhosis, hepatic decompensation, liver transplantation, and liver-related death. Recently, there have been calls to abandon MASH resolution as one of the histological endpoints given its dynamic nature[50], the substantial observer variability in its evaluation[51], and the lack of association with long-term clinical outcomes[52]. Moreover, there is increasing recognition of the need to move away from liver biopsy and to adopt NITs for clinical trials. However, there is currently a lack of a robust NIT test for MASH. On the other hand, NITs for fibrosis, such as LSM, have been shown to be a useful marker and capable of predicting long-term clinical outcomes with performance similar to histology.
In early-phase studies (Phases 1 and 2a), MRI-PDFF, ALT, and blood biomarkers of liver fibrosis are often utilized as endpoints. In particular, a 30% or greater relative reduction in MRI-PDFF correlates with improvement in the NAFLD activity score, MASH resolution, and fibrosis improvement[53]. Because hepatic steatosis changes much earlier than fibrosis, these biomarkers allow early readouts to guide drug development. Drawing from lessons learned in drug development for MASLD, NITs may also be similarly used in early-phase studies for MetALD. Furthermore, NITs can be used as a pre-screening tool to identify patients who are likely to have more severe liver disease for screening for Phase 3 studies, thus reducing screen failure rates and avoiding unnecessary liver biopsy in patients with less severe liver disease.
Several key developments occurred in 2025. First, the US FDA indicated openness to consider NITs as surrogate endpoints in MASH trials[54]. To qualify as a “reasonably likely surrogate endpoint,” a biomarker should be biologically and mechanistically plausible for the disease, demonstrate prognostic performance, and exhibit a magnitude of change that predicts a meaningful change in defined clinical outcomes. To this end, a number of NITs have already demonstrated prognostic performance for predicting liver-related events that is similar to or superior to histological fibrosis staging[55,56]. In particular, changes in LSM by VCTE and MRE, as well as ELF, further correlate with hepatic decompensation and hepatocellular carcinoma[56,57]. Meanwhile, the US FDA has received letters of intent to qualify VCTE and MRE as reasonably likely surrogate endpoints.
The SYNERGY-Outcomes study (NCT07165028) became the first Phase 3 study to use VCTE and ELF alone (i.e., without liver biopsy) for patient recruitment. The objective is to use NITs to identify patients with “at-risk MASH” and a low likelihood of cirrhosis at baseline. After randomization to receive tirzepatide, retatrutide, or placebo, the patients will be followed prospectively for liver-related events. If VCTE and ELF results suggest that the patient has progressed to cirrhosis, this would be confirmed by liver biopsy and treated as the endpoint. Thus, this innovative design reduces the need for serial liver biopsies, although some patients will still require one liver biopsy nonetheless. A biopsy-free design will have to wait until the regulators accept the biomarkers as reasonably likely surrogate endpoints. Theoretically, when these reasonably likely surrogate endpoints are further demonstrated to correlate well with clinical outcomes in Phase 3 trials, they will become validated surrogate endpoints and can be used directly for drug approval [Figure 1]. The use of NITs, when accepted, can simplify and accelerate the clinical phase of drug development by replacing liver biopsy and overcoming its many limitations. Furthermore, the lessons learned from clinical trials can provide guidance on the use of NITs for personalized monitoring strategies in the real-world setting.
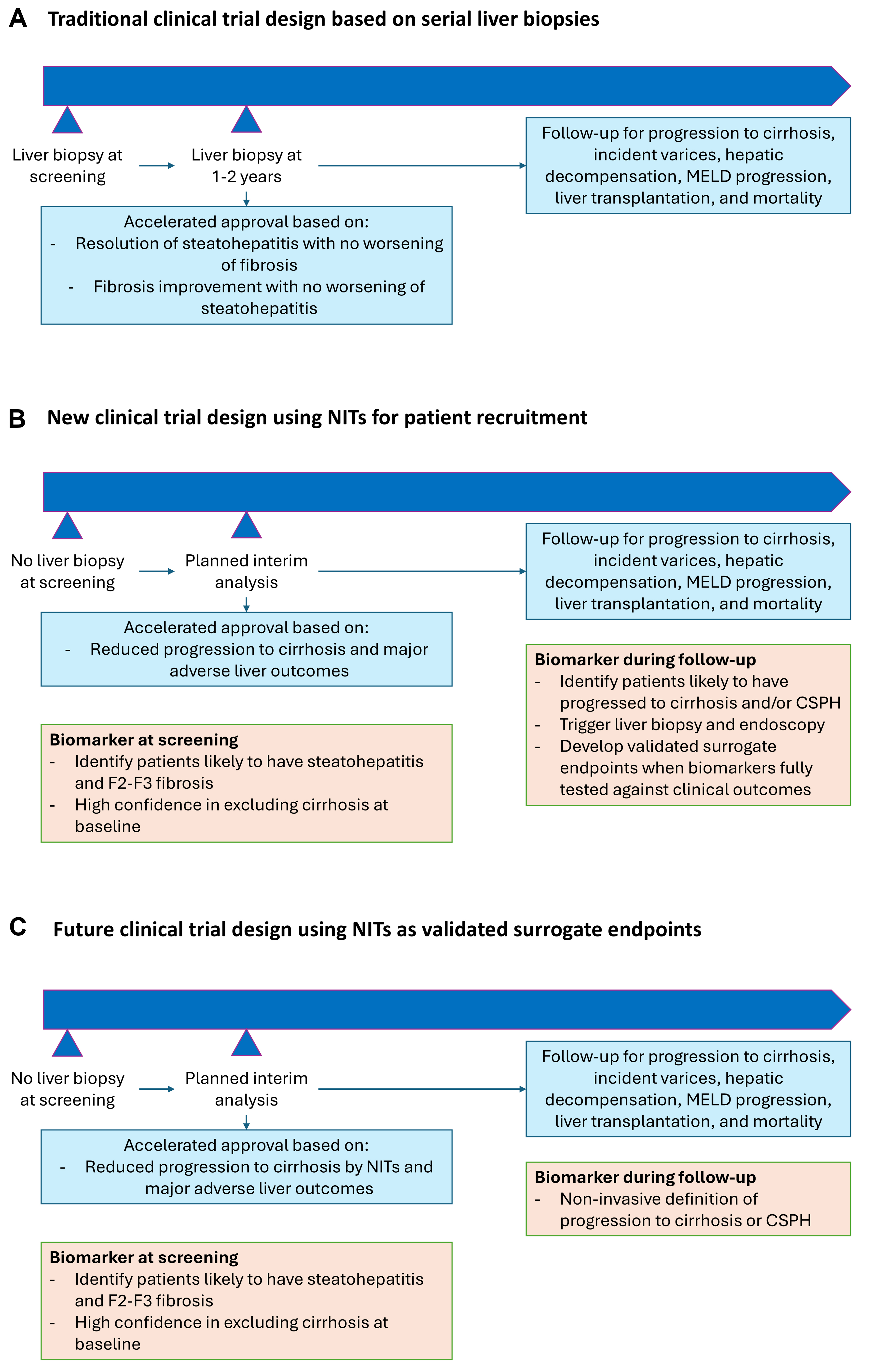
Figure 1. Evolution of clinical trial design for steatotic liver disease. (A) The traditional clinical trial design for MASH requires the use of serial liver biopsies for accelerated drug approval when MASH resolution and fibrosis improvement are achieved. The same trial or a separate trial is needed to demonstrate an improvement in “hard” clinical outcomes during long-term follow-up; (B) A new clinical trial design that can be applied to MASH and MetALD involves the use of NITs alone to identify patients with steatohepatitis and F2-F3 fibrosis, assuming that the tests are sufficient to exclude cirrhosis at baseline. During follow-up, in addition to collecting data on hepatic decompensation and liver-related death, NITs are used to identify patients who have likely progressed to cirrhosis. The latter is then confirmed by liver biopsy and can be counted as a clinical endpoint; (C) When one or more NITs have become validated surrogate endpoints, an entirely biopsy-free clinical trial design becomes possible. Drug approval can then depend solely on NIT response. CSPH: clinically significant portal hypertension; MELD: model for end-stage liver disease; MetALD: metabolic dysfunction-associated alcohol-related liver disease; MASH: metabolic dysfunction-associated steatohepatitis; NITs: noninvasive tests.
A number of issues deserve consideration. When applying the same concepts in MetALD, the impact of fluctuating alcohol consumption on NITs should be scrutinized, especially when changes in NITs become the basis for determining treatment response. Additionally, it is important to remember that MetALD is not just a liver disease but is also related to alcohol consumption. The amount and pattern of alcohol consumption, as measured by validated questionnaires and alcohol biomarkers such as PEth, should at least be a secondary endpoint. This is particularly relevant as glucagon-like peptide-1 receptor agonists (GLP-1RAs) have demonstrated potent effects not only on MASH but also on alcohol craving[5,58]. On the other hand, some NITs, most notably VCTE, are confounded by adiposity. Thus, liver stiffness might decrease significantly during GLP-1RA treatment even in the absence of fibrosis improvement[59].
CONCLUSION AND FUTURE DIRECTION
While data on the performance of NITs in MetALD are currently limited compared to MASLD and ALD, the existing evidence suggests these tools remain effective across the disease spectrum. However, heavy alcohol intake from episodic binge drinking can impair NIT accuracy. Incorporating validated binge assessments and requiring a minimum alcohol-free interval prior to testing may mitigate these issues. While cross-sectional diagnostic performance appears adequate, future research must determine how dynamic changes in alcohol consumption affect NITs when used as longitudinal monitoring or response biomarkers. A key priority for future research is the development of MetALD-specific prognostic scores. Such tools would better identify high-risk patients and help clinicians prioritize interventions - balancing alcohol cessation efforts with cardiometabolic optimization. For years, the histological response of MASH resolution and fibrosis improvement has been the only reasonably likely surrogate endpoint used for accelerated drug approval. The continued reliance on histology is increasingly questioned, as current data suggest that NITs offer comparable prognostic value for liver-related events. While histological fibrosis stage predicts liver-related outcomes[60], data on the prognostic value of histological changes are even scarcer than those for NITs. Additionally, the intra-observer and interobserver variability in histological assessment is substantial, especially when serial samples are examined for response to treatment[51]. Thus, everything being equal, the decision to rely on the more invasive surrogate marker in clinical trials has subjected tens of thousands of patients to the discomfort and risk of repeated liver biopsies for no good reason. As the regulatory pathway for MetALD drug development is still being established, stakeholders have a unique opportunity to adopt more patient-centric, biopsy-free frameworks that could accelerate the delivery of new therapies.
DECLARATIONS
Authors’ contributions
Conceptualized the manuscript: Chan WK
Contributed to section(s) of the manuscript: Chan WK, Liu K, Goh GBB, Wong VWS
Collated the sections and prepared the draft manuscript: Chan WK
Reviewed the draft manuscript, contributed to important intellectual content, and approved the final manuscript: Chan WK, Liu K, Goh GBB, Wong VWS
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool Google Gemini (Version 3.0, 2025-11-18) was used to generate some component graphics for the Graphical Abstract. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
Chan WK has served as a consultant or advisory board member for Abbott, AbbVie, Boehringer Ingelheim, IPSEN, Kowa, Novo Nordisk, Roche and Zuellig Pharma, a speaker for Abbott, Echosens, Hisky Medical, Novo Nordisk, Roche and Viatris, and received research grant from Abbott and Roche. Goh GBB served as a consultant or advisory board member for Roche, MSD, Novo Nordisk, Boehringer Ingelheim and Kowa; and a speaker for Echosens, Viatris, Abbott, Gilead Science and Novo Nordisk. Liu K has no conflict of interest to declare. Wong VWS has served as a consultant or advisory board member for AbbVie, Altimmune, AstraZeneca, Boehringer Ingelheim, Echosens, Eli Lilly, Gilead Sciences, Merck, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, TARGET PharmaSolutions; a speaker for Abbott, AbbVie, AstraZeneca, Echosens, Gilead Sciences, Novo Nordisk; an independent non-executive director for Furui; and a co-founder for Illuminatio Medical Technology. Wong VWS has received a research grant from Gilead Sciences. Wong VWS is an Editorial Board Member of Metabolism and Target Organ Damage. Wong VWS was not involved in any steps of the editorial process, notably including reviewer selection, manuscript handling, and decision-making.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Rinella ME, Lazarus JV, Ratziu V, et al.; NAFLD Nomenclature consensus group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78:1966-86.
2. Cusi K, Abdelmalek MF, Apovian CM, et al. Metabolic dysfunction-associated steatotic liver disease (MASLD) in people with diabetes: the need for screening and early intervention. a consensus report of the American diabetes association. Diabetes Care. 2025;48:1057-82.
3. Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13:221-62.
4. Harrison SA, Bedossa P, Guy CD, et al.; MAESTRO-NASH Investigators. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390:497-509.
5. Sanyal AJ, Newsome PN, Kliers I, et al.; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392:2089-99.
6. Chan WK, Wong VW, Adams LA, Nguyen MH. MAFLD in adults: non-invasive tests for diagnosis and monitoring of MAFLD. Hepatol Int. 2024;18:909-21.
7. Leal-lassalle H, Estévez-vázquez O, Cubero FJ, Nevzorova YA. Metabolic and alcohol-associated liver disease (MetALD): a representation of duality. npj Gut Liver. 2025;2:14.
8. Arab JP, Díaz LA, Rehm J, et al. Metabolic dysfunction and alcohol-related liver disease (MetALD): position statement by an expert panel on alcohol-related liver disease. J Hepatol. 2025;82:744-56.
9. Hernaez R, Lazo M, Bonekamp S, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 2011;54:1082-90.
10. Wu S, Pan J, Song M, et al. Performance of magnetic resonance imaging and ultrasound for identifying the different degrees of hepatic steatosis: a systematic review and meta-analysis. Acad Radiol. 2025;32:6528-40.
11. Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. 2024;81:492-542.
12. Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of alcohol-related liver disease. J Hepatol. 2018;69:154-81.
13. Dulai PS, Singh S, Patel J, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology. 2017;65:1557-65.
14. Vali Y, Lee J, Boursier J, et al.; Liver Investigation: Testing Marker Utility in Steatohepatitis (LITMUS) consortium investigators. Biomarkers for staging fibrosis and non-alcoholic steatohepatitis in non-alcoholic fatty liver disease (the LITMUS project): a comparative diagnostic accuracy study. Lancet Gastroenterol Hepatol. 2023;8:714-25.
15. Vali Y, Lee J, Boursier J, et al.; LITMUS systematic review team(†). Enhanced liver fibrosis test for the non-invasive diagnosis of fibrosis in patients with NAFLD: a systematic review and meta-analysis. J Hepatol. 2020;73:252-62.
16. Selvaraj EA, Mózes FE, Jayaswal ANA, et al.; LITMUS Investigators. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: a systematic review and meta-analysis. J Hepatol. 2021;75:770-85.
17. Newsome PN, Sasso M, Deeks JJ, et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: a prospective derivation and global validation study. Lancet Gastroenterol Hepatol. 2020;5:362-73.
18. Sanyal AJ, Foucquier J, Younossi ZM, et al. Enhanced diagnosis of advanced fibrosis and cirrhosis in individuals with NAFLD using FibroScan-based Agile scores. J Hepatol. 2023;78:247-59.
19. Ferraioli G, Barr RG, Berzigotti A, et al. WFUMB guidelines/guidance on liver multiparametric ultrasound. Part 2: guidance on liver fat quantification. Ultrasound Med Biol. 2024;50:1088-98.
20. Eslam M, Fan JG, Yu ML, et al. The Asian Pacific association for the study of the liver clinical practice guidelines for the diagnosis and management of metabolic dysfunction-associated fatty liver disease. Hepatol Int. 2025;19:261-301.
21. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77:1797-835.
22. de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C; Baveno VII Faculty. Baveno VII - renewing consensus in portal hypertension. J Hepatol. 2022;76:959-74.
23. Oh JH, Ahn SB, Cho S, Nah EH, Yoon EL, Jun DW. Diagnostic performance of non-invasive tests in patients with MetALD in a health check-up cohort. J Hepatol. 2024;81:772-80.
24. Díaz LA, Tavaglione F, Mittal N, et al. Noninvasive pathway for stratifying fibrosis in suspected metabolic dysfunction and alcohol-associated liver disease (MetALD). Hepatol Commun. 2025;9:e0718.
25. Torp N, Israelsen M, Johansen S, et al. MetALD: diagnosis and prognosis with non-invasive tests. Aliment Pharmacol Ther. 2025;62:990-1002.
26. Johansen S, Thiele M, Krag A. Non-invasive tests for MetALD and alcohol-related liver disease. JHEP Rep. 2025;7:101569.
27. Kjærgaard K, Yeoman JM, Eriksen PL, et al. Binge drinking acutely induces hepatic steatosis which is readily reversible: a real-world observational study in healthy adults. JHEP Rep. 2026;8:101623.
28. Mueller S, Millonig G, Sarovska L, et al. Increased liver stiffness in alcoholic liver disease: differentiating fibrosis from steatohepatitis. World J Gastroenterol. 2010;16:966-72.
29. Kanwal F, Neuschwander-Tetri BA, Loomba R, Rinella ME. Metabolic dysfunction-associated steatotic liver disease: update and impact of new nomenclature on the American Association for the Study of Liver Diseases practice guidance on nonalcoholic fatty liver disease. Hepatology. 2024;79:1212-9.
30. Vaz J, Nasr P, Helander A, et al. Phosphatidylethanol levels distinguish steatotic liver disease subgroups and are associated with risk of major liver outcomes. J Hepatol. 2025;83:1011-22.
31. Li M, Chen W, Deng Y, Xie W. Impacts of cardiometabolic risk factors and alcohol consumption on all-cause mortality among MASLD and its subgroups. Nutr Metab Cardiovasc Dis. 2024;34:2085-94.
32. Liu J, Xiao S, Hu S, et al. Dissecting metabolic dysfunction- and alcohol-associated liver disease (MetALD) using proteomic and metabolomic profiles. J Hepatol. 2025;83:1035-45.
33. Singal AK, Shah VH, Malhi H. Emerging targets for therapy in ALD: lessons from NASH. Hepatology. 2024;80:223-37.
34. Tamaki N, Kimura T, Wakabayashi SI, et al. Long-term clinical outcomes in steatotic liver disease and incidence of liver-related events, cardiovascular events and all-cause mortality. Aliment Pharmacol Ther. 2024;60:61-9.
35. Kwak M, Kim HS, Jiang ZG, et al. MASLD/MetALD and mortality in individuals with any cardio-metabolic risk factor: a population-based study with 26.7 years of follow-up. Hepatology. 2025;81:228-37.
36. Celsa C, Pennisi G, Tulone A, et al. Risk of hepatic and extrahepatic outcomes associated with metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction and alcohol-associated steatotic liver disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2025;10:998-1012.
37. Li Z, Shen Y, Li Z, Cao D, Hu Y. Is MetALD an independent risk factor of all-cause mortality? A meta-analysis of 164,694 individuals from the real world. J Hepatol. 2025;82:e95-7.
38. Sripongpun P, Kaewdech A, Udompap P, Kim WR. Characteristics and long-term mortality of individuals with MASLD, MetALD, and ALD, and the utility of SAFE score. JHEP Rep. 2024;6:101127.
39. Castera L, Rinella ME, Tsochatzis EA. Noninvasive assessment of liver fibrosis. N Engl J Med. 2025;393:1715-29.
40. Sudhinaraset M, Wigglesworth C, Takeuchi DT. Social and cultural contexts of alcohol use: influences in a social-ecological framework. Alcohol Res. 2016;38:35-45.
41. Torp N, Israelsen M, Thiele M, Rinella ME, Krag A. Phosphatidylethanol in steatotic liver disease. J Hepatol. 2025;83:1189-203.
42. Krag A, Torp N, Younossi ZM, Israelsen M. Reporting discrepancy of alcohol intake affecting estimated prevalence of MetALD and ALD. Lancet Gastroenterol Hepatol. 2025;10:282-4.
43. Lee JH, Ahn SH, Park J, et al. Misclassification of Alcohol Use Disorder in MASLD and MetALD: Prevalence, Clinical Characteristics, and Outcomes. Gut Liver. 2025;19:735-45.
44. Ayares G, Diaz LA, Idalsoaga F, et al. MetALD: new perspectives on an old overlooked disease. Liver Int. 2025;45:e70017.
45. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption--II. Addiction. 1993;88:791-804.
46. Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007;31:1208-17.
47. O’Brien CP. The CAGE questionnaire for detection of alcoholism: a remarkably useful but simple tool. JAMA. 2008;300:2054-6.
48. Arab JP, Izzy M, Leggio L, Bataller R, Shah VH. Management of alcohol use disorder in patients with cirrhosis in the setting of liver transplantation. Nat Rev Gastroenterol Hepatol. 2022;19:45-59.
49. Tavaglione F, Díaz LA, Ajmera V, et al. Clinical utility of phosphatidylethanol to detect underreported alcohol use and enhance steatotic liver disease subclassification. J Hepatol. 2025;83:1023-34.
50. Kleiner DE, Brunt EM, Wilson LA, et al.; Nonalcoholic Steatohepatitis Clinical Research Network. Association of histologic disease activity with progression of nonalcoholic fatty liver disease. JAMA Netw Open. 2019;2:e1912565.
51. Davison BA, Harrison SA, Cotter G, et al. Suboptimal reliability of liver biopsy evaluation has implications for randomized clinical trials. J Hepatol. 2020;73:1322-32.
52. Hagström H, Nasr P, Ekstedt M, et al. Fibrosis stage but not NASH predicts mortality and time to development of severe liver disease in biopsy-proven NAFLD. J Hepatol. 2017;67:1265-73.
53. Stine JG, Munaganuru N, Barnard A, et al. Change in MRI-PDFF and histologic response in patients with nonalcoholic steatohepatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2021;19:2274-83.e5.
54. Anania FA, Hager R, Higgins K, Makar GA, Siegel J, Tran TT. Non-invasive tests: establishing efficacy for metabolic dysfunction-associated steatohepatitis beyond the biopsy-Current perspectives from the Division of Hepatology and Nutrition, US Food and Drug Administration. Hepatology. 2025;Epub ahead of print.
55. Mózes FE, Lee JA, Vali Y, et al.; LITMUS investigators. Performance of non-invasive tests and histology for the prediction of clinical outcomes in patients with non-alcoholic fatty liver disease: an individual participant data meta-analysis. Lancet Gastroenterol Hepatol. 2023;8:704-13.
56. Lin H, Lee HW, Yip TC, et al.; VCTE-Prognosis Study Group. Vibration-controlled transient elastography scores to predict liver-related events in steatotic liver disease. JAMA. 2024;331:1287-97.
57. Gawrieh S, Vilar-Gomez E, Wilson LA, et al.; NASH Clinical Research Network. Increases and decreases in liver stiffness measurement are independently associated with the risk of liver-related events in NAFLD. J Hepatol. 2024;81:600-8.
58. Klausen MK, Thomsen M, Wortwein G, Fink-Jensen A. The role of glucagon-like peptide 1 (GLP-1) in addictive disorders. Br J Pharmacol. 2022;179:625-41.
59. Wai-Sun Wong V, Anstee QM, Nitze LM, et al. FibroScan-aspartate aminotransferase (FAST) score for monitoring histological improvement in non-alcoholic steatohepatitis activity during semaglutide treatment: post-hoc analysis of a randomised, double-blind, placebo-controlled, phase 2b trial. EClinicalMedicine. 2023;66:102310.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.