


From platforms to pathways: imaging innovation, quantitative biomarkers, and clinical translation in hepatocellular carcinoma
 0
0 Abstract
Imaging is central to nearly every stage of hepatocellular carcinoma (HCC) management, from surveillance and noninvasive diagnosis to staging, locoregional therapy planning, treatment response assessment, and recurrence monitoring. Recent progress begins with imaging hardware but depends just as much on acquisition design, reconstruction, quantification, harmonization, and workflow integration. This narrative review examines how ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and nuclear or hybrid imaging have changed HCC care, while separating clinically established tools from technologies that remain largely translational. Ultrasound has advanced beyond screening through contrast-enhanced ultrasound (CEUS), Kupffer-phase agents, elastography, and fusion navigation. CT has progressed through spectral imaging, deep learning reconstruction, and cone-beam guidance, whereas photon-counting CT remains promising but early. MRI has consolidated its role through 3T platforms, multichannel coils, accelerated acquisitions, hepatobiliary contrast agents, diffusion-based imaging, magnetic resonance elastography (MRE), and abbreviated protocols. Positron emission tomography remains constrained by tracer biology in early HCC, although novel tracers and positron emission tomography (PET)/MRI broaden selected applications. Across modalities, imaging advances are most useful when acquisition and biomarker extraction are reproducible enough to support the Liver Imaging Reporting and Data System (LI-RADS), treatment response assessment, and downstream clinical decisions. Evidence is strongest for CEUS, gadoxetic acid-enhanced MRI, MRE for selected risk questions, and image-guided interventional platforms, whereas spectral CT has growing selected-use evidence but still requires broader standardization of quantitative thresholds. By contrast, radiomics, deep learning, advanced diffusion models, photon-counting CT, and theranostic-oriented molecular imaging still face important barriers related to external validity, harmonization, and clinical qualification.
Keywords
INTRODUCTION
Hepatocellular carcinoma (HCC) sits at the intersection of liver cancer biology and chronic liver disease. GLOBOCAN 2022 estimated approximately 866,000 incident liver cancers and 759,000 deaths worldwide, which keeps earlier detection and dependable follow-up at the center of HCC care[1]. Most HCC develops in cirrhosis or other chronic liver disease, so patients often enter an imaging pathway before a tumor is confirmed[2,3]. In selected at-risk patients, dynamic contrast-enhanced imaging can establish the diagnosis without biopsy, map tumor burden, guide locoregional therapy, and monitor response or recurrence[4-7].
The problem is not simply whether ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) can produce sharper images. HCC care depends on whether images are acquired at the right phase, reconstructed consistently, quantified reproducibly, and reported in language that clinicians can use. The Liver Imaging Reporting and Data System (LI-RADS), modified Response Evaluation Criteria in Solid Tumors (mRECIST), and treatment response algorithms have helped standardize parts of this pathway[8,9]. Previous guidelines and modality-specific frameworks have often summarized HCC imaging by individual modality or reporting system[2-4,8]. That organization is useful, but it can hide the practical question this review addresses: which platform advances actually reduce uncertainty during surveillance, diagnosis, treatment planning, response assessment, or recurrence monitoring?
Literature selection and review scope
This narrative review uses a platform-to-pathway structure to answer that question. It follows imaging progress from hardware and acquisition through reconstruction, quantitative biomarkers, standardization, and clinical translation, with attention to where the evidence is mature and where it remains early. The review was based on targeted searches of PubMed, Web of Science, and Google Scholar, prioritizing publications from January 2018 to May 2026 and earlier landmark guidelines, consensus statements, response criteria, and technical validation studies when needed. Search concepts included HCC, contrast-enhanced ultrasound (CEUS), spectral CT, photon-counting CT, gadoxetic acid-enhanced MRI, magnetic resonance elastography (MRE), PET, fibroblast activation protein inhibitor (FAPI), quantitative European Association for the Study of the Liver (qEASL), radiomics, artificial intelligence (AI), and treatment response. We prioritized clinical guidelines, consensus documents, systematic reviews, meta-analyses, multicenter or prospective studies, public datasets, and representative technical studies with clinically relevant HCC endpoints[2-9].
WHY HCC REMAINS UNIQUELY IMAGING-DEPENDENT ACROSS THE CLINICAL PATHWAY
HCC remains uniquely imaging-dependent because each major clinical decision is conditioned on serial imaging evidence. Surveillance in high-risk populations still begins with ultrasound, often with alpha-fetoprotein (AFP) as an adjunct, despite the well-recognized sensitivity ceiling of ultrasound alone for early-stage disease[2,3,10,11]. Once a nodule is detected, multiphasic CT, MRI, or CEUS can characterize arterial phase hyperenhancement, washout, capsule appearance, and ancillary features that drive noninvasive diagnosis in at-risk patients[4,5,8]. The same patient may then undergo MRI for staging, ultrasound or cone-beam CT (CBCT) guidance for therapy, and structured imaging-based response assessment after embolization, ablation, or radiation-related treatment[6,7,9].
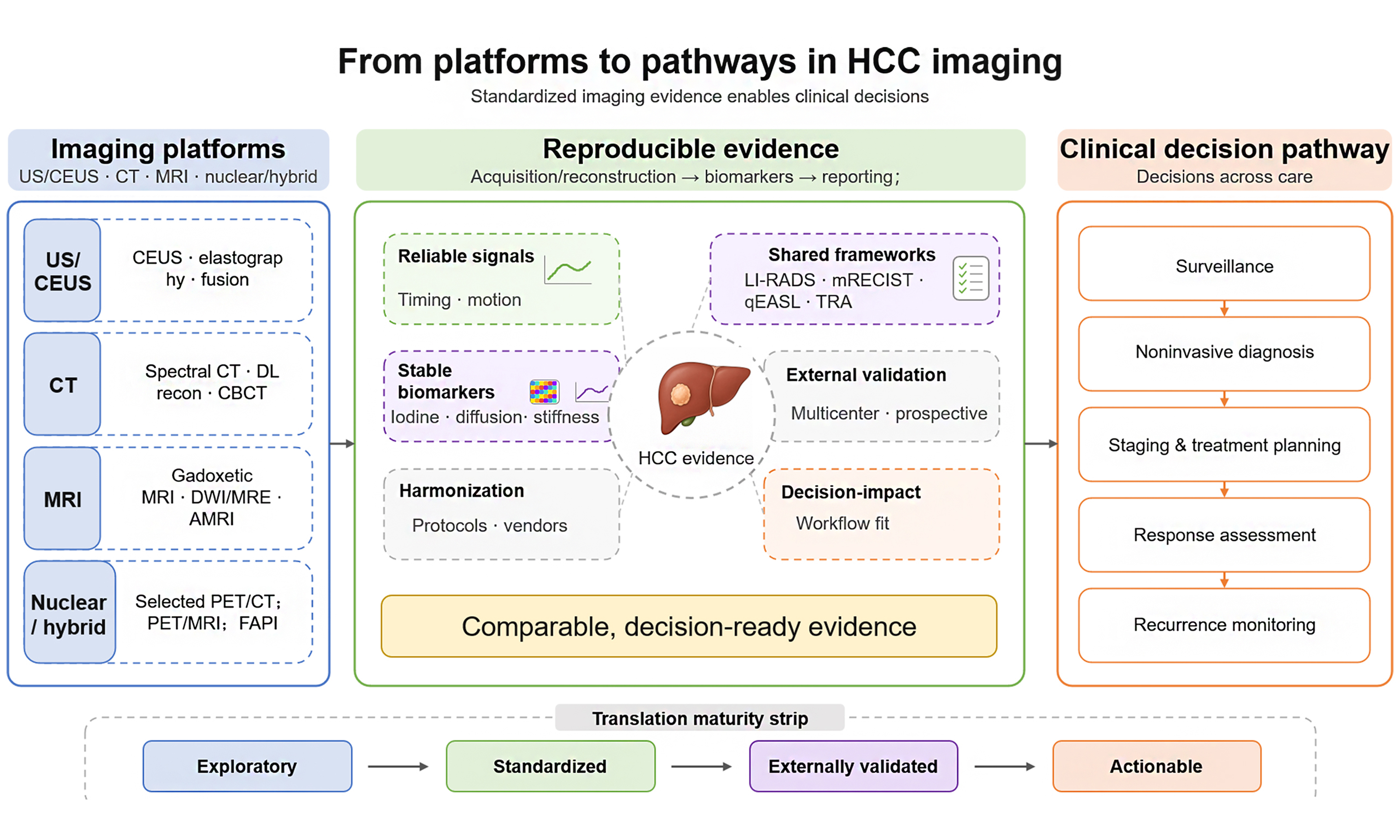
This longitudinal role makes HCC an instructive setting for viewing imaging as a continuum of linked steps rather than as a series of disconnected tests [Figure 1]. Upstream hardware governs whether raw data are sensitive, fast, and stable enough. Acquisition and reconstruction determine whether relevant vascular and tissue contrast is captured, while quantitative extraction and reporting determine whether findings remain comparable across readers and centers. Only then can imaging serve as a reliable basis for treatment planning or response assessment. In practice, the technologies that matter most are those that reduce uncertainty at one or more of these interfaces.
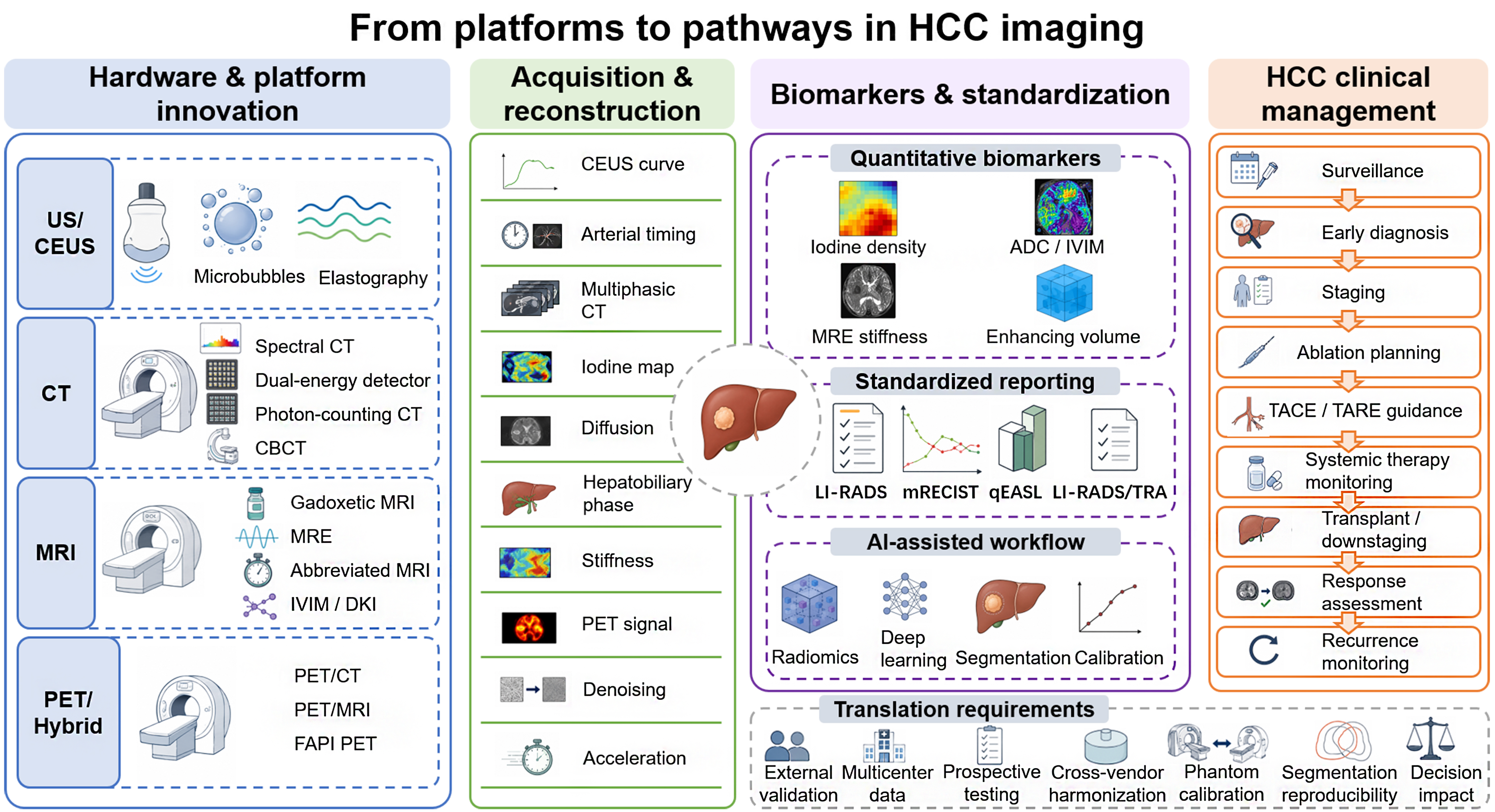
Figure 1. Conceptual pipeline for HCC imaging translation. Platform innovation at the hardware level enables acquisition and reconstruction strategies that determine whether vascular, cellular, and microenvironmental signals can be converted into quantitative biomarkers, standardized reporting, and clinically actionable decisions across surveillance, diagnosis, treatment guidance, response assessment, and recurrence monitoring. HCC: Hepatocellular carcinoma; US: ultrasound; CEUS: contrast-enhanced ultrasound; CT: computed tomography; MRI: magnetic resonance imaging; MRE: magnetic resonance elastography; IVIM: intravoxel incoherent motion; DKI: diffusion kurtosis imaging; CBCT: cone-beam computed tomography; PET: positron emission tomography; PET/CT: positron emission tomography/computed tomography; PET/MRI: positron emission tomography/magnetic resonance imaging; FAPI: fibroblast activation protein inhibitor; ADC: apparent diffusion coefficient; LI-RADS: Liver Imaging Reporting and Data System; mRECIST: modified Response Evaluation Criteria in Solid Tumors; qEASL: quantitative European Association for the Study of the Liver; TACE: transarterial chemoembolization; TARE: transarterial radioembolization; TRA: treatment response algorithm; AI: artificial intelligence.
HARDWARE AND PLATFORM EVOLUTION ACROSS MAJOR MODALITIES
Platform-level advances have not affected all modalities equally, and their value is not defined by novelty alone. Representative strengths and unresolved issues are summarized in Table 1.
Representative platform-level advances in HCC imaging and their clinical readiness
| Modality/innovation | Main HCC decision point | Clinical readiness | Key contribution | Main limitation or implementation barrier | Representative references |
| US surveillance | Population-scale surveillance and first-line detection gateway | Established clinical use | Accessible surveillance gateway; US LI-RADS v2024 standardizes technique, visualization score, and triage | Operator dependence; poor acoustic windows; limited early-stage sensitivity | [2,3,5,10,11] |
| CEUS/CEUS LI-RADS | Problem solving for indeterminate nodules; vascular characterization | Established clinical use/Selected/emerging use | Real-time arterial capture and washout; problem solving when CT/MRI is limited | Limited whole-liver staging; variable agent access, reimbursement, and expertise | [8,16-20] |
| Kupffer-phase CEUS/Sonazoid workflow | Small-lesion conspicuity and selected surveillance-adjacent workflows | Selected/emerging use | Delayed Kupffer phase improves lesion conspicuity in perfluorobutane-based workflows | Not interchangeable with blood-pool agents; limited global availability and algorithm portability | [21-25] |
| Elastography | Background liver risk context; exploratory tumor/peritumor biology | Established clinical use/Selected/emerging use | Adds liver stiffness and microenvironmental context beyond morphology | Not a standalone HCC diagnostic test; stiffness is affected by inflammation, congestion, cholestasis, and technique | [26-29] |
| Fusion US/image-guided ablation | Ablation planning and intraprocedural targeting | Selected/emerging use | Improves targeting of lesions poorly visible on conventional US and links preprocedural imaging to treatment execution | Requires registration expertise, compatible equipment, and careful quality control | [30-32] |
| Multiphasic CT | Noninvasive diagnosis, staging, vascular mapping, and routine follow-up | Established clinical use | Fast, robust, widely available; supports arterial, portal venous, and delayed-phase assessment | Radiation and iodinated contrast exposure; phase timing and reconstruction affect quantitative biomarkers | [2-4,33,34] |
| Spectral/dual-energy CT | Lesion conspicuity; viable enhancement after locoregional therapy | Selected/emerging use | Low-keV images and iodine maps can improve visualization of subtle hyperenhancement and residual viability | No universal HCC thresholds; scanner/vendor dependence and harmonization remain incomplete | [35-39] |
| Deep learning CT reconstruction | Repeated multiphasic follow-up with lower dose or higher image quality | Selected/emerging use | Can reduce noise and dose while maintaining diagnostic confidence | Changes noise texture and edge behavior; radiomics and quantitative biomarkers require revalidation | [40-42] |
| Photon-counting CT | Small lesion detection; spectral/low-dose liver imaging | Research/translational stage | Higher spatial resolution and energy separation may improve small-lesion detection and dose efficiency | HCC-specific clinical evidence remains early and concentrated in expert settings | [43,44] |
| Perfusion CT | Tumor vascularity and antiangiogenic or locoregional response research | Research/translational stage | Can capture dynamic vascular parameters beyond static multiphasic enhancement | Radiation dose, protocol heterogeneity, and lack of harmonized thresholds limit routine use | [45,46] |
| CBCT-assisted TACE/TARE | TACE/TARE planning, feeding-artery detection, target coverage confirmation | Established clinical use/Selected/emerging use | Turns the angiography suite into a 3D treatment-planning environment and supports superselective therapy | Requires CBCT-equipped interventional suite, expertise, and dose/contrast management | [47-50] |
| Gadoxetic acid-enhanced MRI | Small-lesion diagnosis, staging, recurrence surveillance, transplant/downstaging assessment | Established clinical use | Combines vascular phases with hepatobiliary-phase biology; high sensitivity for small/equivocal lesions | Cost, time, motion artifacts, hepatobiliary-phase quality, and contrast-specific pitfalls | [2-4,54-57] |
| DWI/ADC | Ancillary lesion conspicuity and cellularity-related assessment | Established clinical use/Selected/emerging use | DWI is broadly available and ADC offers a simple quantitative diffusion metric | ADC thresholds vary with protocol, b-values, motion, and scanner platform | [58,59] |
| IVIM/DKI | Tumor biology, perfusion, microstructure, and aggressiveness research | Research/translational stage | May capture perfusion-related diffusion and non-Gaussian tissue heterogeneity | Fitting instability, acquisition burden, vendor dependence, and limited external validation | [60,61] |
| MRE | Liver stiffness, background liver risk, selected prognosis questions | Selected/emerging use | Highly reproducible liver stiffness biomarker; complements dynamic contrast-enhanced diagnosis | More useful for liver background and risk context than lesion diagnosis; hardware/workflow constraints | [62-64] |
| AMRI | Alternative surveillance in patients with inadequate US or high risk | Selected/emerging use | Workflow innovation that can bring MRI closer to surveillance-compatible use | Patient selection, cost, throughput, contrast strategy, and local availability determine feasibility | [54,65-67] |
| FDG/acetate/choline PET | Selected staging dilemmas, extrahepatic disease, recurrence, biologic characterization | Selected/emerging use | Whole-body biologic characterization beyond morphology; dual-tracer approaches may improve selected assessments | FDG sensitivity is low in well-differentiated HCC; tracers are not routine for early intrahepatic diagnosis | [68-71] |
| FAPI PET | Stromal biology, selected staging, and theranostic exploration | Research/translational stage | May visualize biology missed by FDG in selected liver tumors | FAPI uptake is not tumor-specific; HCC outcome validation and guideline qualification remain incomplete | [72,73,94] |
| PET/MRI | Hybrid whole-body and liver-specific problem solving | Selected/emerging use/Research/translational stage | Combines metabolic information with superior liver MRI contrast in one examination | Cost, workflow complexity, attenuation correction, and uncertain routine management impact | [74] |
Ultrasound
Ultrasound remains the default entry point into the HCC pathway because it is accessible, repeatable, inexpensive, and free of ionizing radiation. The surveillance challenge, however, goes beyond visualizing the liver: small, often subtle nodules must be detected consistently enough to justify downstream work-up. Contrast-specific workflows such as Sonazoid defect-reperfusion imaging show how ultrasound platforms can move beyond morphology in selected HCC settings[12]. Contemporary Doppler and microvascular flow imaging technologies further improve sensitivity to slow flow without contrast[13-15]. These upgrades are meaningful, but they reduce rather than eliminate operator dependence.
CEUS has been the most consequential shift because it turns ultrasound from a morphology-driven surveillance test into a real-time hemodynamic imaging tool. Continuous observation of arterial fill-in and subsequent washout is especially valuable when CT or MRI may miss the critical arterial window, or when a small indeterminate nodule requires real-time problem solving[16-18]. CEUS LI-RADS and subsequent reviews have demonstrated high specificity in the intended at-risk population, although diagnostic behavior still depends on contrast-agent type, lesion size, and reader expertise[8,19,20]. The 2024 CEUS nonradiation treatment response algorithm is also conceptually important because it extends ultrasound from diagnosis into structured post-treatment assessment, particularly after ablation or other nonradiation therapies[7].
Kupffer-phase agents, especially perfluorobutane formulations, further expand ultrasound by adding a delayed reticuloendothelial phase that improves conspicuity of lesions lacking normal Kupffer cell function[21-23]. For small or atypical nodules, this may improve detection and sometimes classification. It also complicates direct transfer of CEUS algorithms across regions, because Sonazoid-based workflows are not interchangeable with blood-pool microbubble workflows[24,25]. Elastography adds another dimension. Liver stiffness is already clinically relevant for chronic liver disease severity, and tumoral or peritumoral stiffness has been explored as a marker of microvascular invasion, recurrence risk, or aggressive biology[26-29]. The most durable clinical contribution of elastography in HCC is probably risk contextualization rather than lesion diagnosis.
Fusion navigation has expanded what ultrasound can accomplish during treatment. Registration of real-time ultrasound with CT or MRI, often with electromagnetic tracking, allows poorly conspicuous tumors to be targeted for ablation and shortens the distance between preprocedural planning and intraprocedural execution[30-32]. In HCC, modern ultrasound is best viewed as a flexible platform spanning surveillance, problem solving, and intervention.
CT
Multiphasic CT remains a foundational modality for diagnosis, staging, vascular mapping, and post-treatment follow-up because it combines speed, consistency, and broad availability. Much of its clinical reliability comes from hardware evolution that is easy to overlook: faster gantry rotation, wider detector coverage, better z-axis resolution, and improved dose efficiency make it more likely that arterial, portal venous, and delayed phases are acquired at the right time and with consistent whole-liver coverage[33,34]. For HCC, this temporal reliability matters as much as nominal spatial resolution.
Dual-energy and spectral CT have moved CT beyond attenuation measurement toward material-sensitive imaging. Low-keV virtual monochromatic images can accentuate hypervascular lesions, iodine maps can clarify viable enhancement after locoregional therapy, and virtual noncontrast images can sometimes reduce the need for true unenhanced acquisitions[35-37]. Evidence in HCC is strongest where spectral data augment visual judgment rather than replace it. Iodine density and low-keV reconstructions can increase lesion-to-liver contrast or make subtle residual enhancement more conspicuous, but universally accepted thresholds for diagnosis or response are lacking[38,39].
Reconstruction has been the second major CT frontier. Deep learning reconstruction and related hybrid approaches allow lower-dose multiphasic examinations while preserving or improving low-contrast detectability, an especially relevant advantage in a population requiring repeated follow-up imaging[40-42]. The caveat is that reconstruction is no longer a neutral postprocessing step. When noise texture and edge behavior change, quantitative features and radiomics signatures may also shift, so biomarker portability cannot be assumed across reconstruction generations.
Photon-counting CT is the most visible current hardware leap. By directly counting photons and preserving energy information at the detector level, it promises higher spatial resolution, better spectral separation, and improved dose utilization[43]. Early liver data are encouraging, including better conspicuity of small lesions and improved spectral image quality, but HCC-specific evidence remains preliminary and concentrated in expert centers[44]. A similar caution applies to perfusion CT. It can capture tumor vascularity and antiangiogenic response more directly than static multiphasic CT, yet protocol heterogeneity, radiation exposure, and limited harmonization have kept it largely in the research domain[45,46].
By contrast, CBCT has already shown clear procedural value. In transarterial chemoembolization (TACE) or radioembolization, intraprocedural CBCT turns the angiography suite into a three-dimensional imaging environment that can improve feeding-artery detection, confirm target coverage, and support superselective therapy[47-50]. This may be the most clinically mature example of CT technology improving HCC care through treatment execution rather than diagnosis itself.
MRI
MRI has consolidated its central role in HCC because it combines high soft-tissue contrast with the broadest palette of structural and functional tissue characterization. Its evolution has been cumulative rather than singular. The move to 3T systems, multichannel torso coils, and parallel imaging strategies such as sensitivity encoding and generalized autocalibrating partially parallel acquisition increased signal efficiency and shortened acquisitions[51-53]. More recent motion-robust and accelerated dynamic strategies build on this foundation, aiming to preserve arterial-phase fidelity in patients who struggle with breath-holding or have limited physiologic reserve[54].
Hepatobiliary contrast agents, especially gadoxetic acid, are a major reason MRI frequently outperforms CT for small or otherwise equivocal lesions. By combining vascular-phase imaging with delayed hepatocyte uptake, they create a second biologic contrast mechanism that highlights lesions with reduced hepatocellular function[55-57]. This advantage is most compelling in small HCC, borderline nodules, or patients in whom surveillance-detected lesions remain indeterminate after ultrasound or CT. At the same time, hepatobiliary-phase hypointensity is not synonymous with overt HCC, and contrast-specific artifacts or timing pitfalls can weaken arterial-phase interpretation. MRI retains its advantage when all phases, not just one, are interpreted within a standardized framework.
Diffusion-weighted imaging (DWI) is now a core sequence because it increases lesion conspicuity and provides a semiquantitative window into cellularity. Yet the more sophisticated diffusion models that followed, including intravoxel incoherent motion (IVIM) and diffusion kurtosis imaging (DKI), also illustrate how difficult quantitative MRI remains to implement clinically. These methods are biologically attractive because they attempt to separate diffusion from microperfusion or to characterize non-Gaussian diffusion behavior, and they have been associated with grading, microvascular invasion, or aggressive phenotypes in HCC[58-61]. The challenge is robustness: parameter estimates remain sensitive to b-value design, fitting strategy, motion, and vendor implementation.
MRE is further along the maturity curve. It is one of the most reproducible imaging tools for liver stiffness assessment and has already demonstrated value in chronic liver disease and in selected HCC risk or prognosis questions[62-64]. In practice, its most convincing role in HCC is as a background liver and microenvironment biomarker rather than a standalone tumor detection tool.
Abbreviated MRI (AMRI) represents a different type of progress, namely workflow redesign rather than new physics. By selecting a reduced sequence set, sometimes contrast-enhanced and sometimes noncontrast, abbreviated protocols aim to move MRI closer to a surveillance-compatible test for patients in whom ultrasound is likely to underperform[65-67]. The appeal is clear, but AMRI should not be framed as universally superior surveillance. Its value depends on patient selection, local throughput, cost, and which sequences are prioritized. AMRI is therefore as much a pathway innovation as a scanner innovation.
Nuclear and hybrid imaging
Nuclear and hybrid imaging currently occupy a more selective role in HCC than ultrasound, CT, or MRI, but they remain important for biologic characterization and whole-body assessment. The well-known limitation of fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) is its relatively low sensitivity for well-differentiated HCC, which restricts its value for early intrahepatic detection[68-70]. FDG is more useful when biology is less favorable, for example in poorly differentiated tumors, extrahepatic disease, recurrence, or prognosis-related questions.
Alternative tracers such as acetate or choline can complement FDG, and newer FAPI tracers have generated interest because they may visualize stromal biology not captured by FDG alone[71-73]. Here again, tracer innovation has outpaced standard clinical qualification. FAPI uptake is not tumor-specific, theranostic implications in HCC remain exploratory, and most published evidence is based on small cohorts or pooled analyses.
PET/MRI illustrates both the promise and the practical limits of hybrid imaging. It combines metabolic information with superior liver MRI contrast within one examination and can be useful in selected hepatobiliary problem-solving settings, but its routine role remains constrained by cost, workflow complexity, and attenuation-correction challenges[74]. Hardware refinements such as digital detector architectures and improved time-of-flight performance are technically favorable, yet in HCC PET usefulness still depends more on tracer biology than on scanner hardware.
ACQUISITION AND RECONSTRUCTION INNOVATIONS THAT CHANGED DIAGNOSTIC PERFORMANCE
Across modalities, the central technical question in HCC is whether acquisition and reconstruction capture the right biology at the right moment. Raw signal alone is not enough. This is most obvious in arterial-phase imaging. Hyperenhancement remains a key diagnostic and response feature, yet it is easy to miss because it depends on bolus timing, temporal resolution, and motion control. Ultrasound partly escapes this problem through continuous real-time sampling, which helps explain why CEUS is so effective for problem solving indeterminate nodules[16,17]. CT addresses it through speed and reproducible multiphasic timing, increasingly complemented by spectral reconstructions that recover contrast when standard images are borderline[36-39]. MRI relies less on raw speed than on acceleration, parallel imaging, and motion-robust dynamic strategies that trade sequence complexity for more reliable arterial-phase capture[51,52,54].
Reconstruction now deserves equal attention because it changes what counts as an interpretable image. Deep learning reconstruction on CT and AI-assisted acceleration on MRI can reduce noise, shorten acquisitions, and rescue studies that would previously have been nondiagnostic[40,42,54]. The clinical gain is greatest when decision-level performance is preserved, such as maintaining confidence in lower-dose multiphasic CT or making AMRI feasible in frail patients[41,66]. The complication is that reconstruction can also alter texture, sharpness, or apparent enhancement patterns. Biomarkers that depend on intensity distribution, edge definition, or voxelwise heterogeneity therefore require revalidation when acquisition or reconstruction changes.
These issues explain why acquisition and reconstruction should be treated as part of the clinical evidence rather than as invisible vendor engineering. A new detector, acceleration scheme, or reconstruction network becomes clinically meaningful only when it improves the stability of diagnosis, response assessment, or intervention planning. In HCC, where serial comparison is essential, consistency may matter more than maximal image sharpness.
QUANTITATIVE IMAGING, STANDARDIZATION, AND TREATMENT RESPONSE FRAMEWORKS
Quantitative imaging is attractive in HCC because it promises to convert complex vascular and microenvironmental biology into serial, auditable measurements. CEUS time-intensity-curve parameters, CT iodine density, diffusion metrics, stiffness maps, and volumetric enhancement assessments all attempt to move interpretation beyond visual pattern recognition. The recurring problem is that quantitative data are only as useful as their technical stability. Without harmonized acquisition, reconstruction, segmentation, and reporting, thresholds drift across centers and biomarkers remain difficult to qualify for clinical decisions. Relevant standardization frameworks and biomarker classes are summarized in Table 2[39,58,62,75-77].
Standardization frameworks, quantitative biomarkers, and AI/radiomics translation requirements in HCC imaging
| Framework/biomarker class | What it standardizes or measures | Main clinical task | Current readiness | Key limitation | Required next step/translational requirement | Representative references |
| CT/MRI LI-RADS | Major and ancillary imaging features for noninvasive diagnosis in at-risk patients | Diagnosis and multidisciplinary communication | Established clinical use | Depends on acquisition quality and intended population; limited for non-HCC malignancies and non-at-risk patients | Protocol quality assurance, education, transparent reporting, and outcome-linked updates | [4,8,76,77] |
| US LI-RADS | US category, visualization score, technical recommendations, and triage | Surveillance and follow-up triage | Established clinical reporting framework | Persistent operator and visualization variability; inadequate US requires alternative surveillance planning | Risk- and visualization-adapted surveillance pathways, workflow integration, and prospective validation | [5] |
| CEUS LI-RADS | Real-time enhancement pattern, washout timing/intensity, and CEUS category assignment | Problem solving and noninvasive diagnosis in selected at-risk patients | Established clinical use/Selected/emerging use | Agent type, lesion size, reader expertise, and regional availability affect portability | Multicenter datasets, external validation, education, and cross-region implementation studies | [8,19,20] |
| CT/MRI LI-RADS TRA 2024 | Categorical post-LRT viability assessment; nonradiation and radiation-based therapy patterns | Response assessment, retreatment, transplant bridging/downstaging | Established/updated reporting framework | Outcome linkage varies by treatment mechanism; equivocal/nonprogressing categories need clinical validation | Prospective validation with pathology, retreatment decisions, transplant outcomes, and decision-impact studies | [6] |
| CEUS Nonradiation TRA 2024 | Real-time CEUS assessment of viable tumor and post-treatment change after nonradiation LRT or resection | Ablation and nonradiation post-treatment assessment | Selected/emerging standardized framework | Does not cover all radiation-based therapies; local expertise and acoustic windows constrain use | Multicenter validation across ablation techniques, follow-up schedules, and workflow integration | [7] |
| mRECIST | One-dimensional diameter of viable arterial-enhancing tumor rather than total lesion size | Trials and routine response assessment after LRT/systemic therapy | Widely used clinical and trial metric | Geometric simplification; limited for irregular, infiltrative, partially necrotic, or heterogeneous tumors and extrahepatic disease | Harmonized use with RECIST 1.1, LI-RADS TRA, and volumetric adjuncts; decision-impact studies | [9] |
| qEASL/volumetric enhancement assessment | Viable enhancing tumor volume and percentage enhancement change | Quantitative response assessment after TACE/TARE/ablation; research workflows | Promising quantitative adjunct | Segmentation, subtraction registration, enhancement threshold, software, timing, and cross-center calibration dependence | Segmentation reproducibility, prespecified thresholds, external validation, model calibration, and decision-impact studies | [78,92,93] |
| CT iodine density/low-keV spectral CT | Iodine concentration, virtual monochromatic image contrast, and material-sensitive enhancement | Viable enhancement, lesion conspicuity, and response research | Selected/emerging use | Threshold instability across scanners, reconstruction settings, contrast timing, and vendors | Phantom calibration, cross-vendor harmonization, protocol locking, and prospective validation | [35-39] |
| ADC | Apparent diffusion coefficient as a simple diffusion-derived cellularity metric | Ancillary characterization and response/risk research | Established adjunct/Selected-emerging quantitative use | ADC varies with b-values, acquisition, motion, fitting approach, and scanner platform | Protocol harmonization, repeatability studies, external validation, and clinically meaningful endpoints | [58,59] |
| IVIM/DKI | Perfusion-related diffusion and non-Gaussian microstructural diffusion metrics | Tumor biology, aggressiveness, and response research | Research/translational stage | Longer acquisition, model instability, vendor differences, and limited multicenter evidence | Multicenter datasets, phantom calibration, cross-vendor harmonization, and prospective validation | [60,61] |
| MRE stiffness | Background liver stiffness and selected tissue-mechanical risk markers | Risk context, liver background assessment, and selected prognosis questions | Selected/emerging use | More informative for liver background than lesion diagnosis; hardware and workflow constraints | External validation, cross-vendor harmonization, standardized acquisition, and outcome-linked thresholds | [62-64] |
| Radiomics | High-dimensional shape, intensity, texture, and habitat features | MVI/grade/CK19 prediction, recurrence, response, survival, LI-RADS assistance | Research/translational stage | Retrospective single-center designs, unstable labels, data leakage risk, segmentation variability, and feature shift | IBSI-compliant extraction, patient-level splitting, external validation, model calibration, decision-curve analysis, and open reproducible code | [79-85] |
| Deep learning/AI prediction models | End-to-end or feature-learning models for detection, classification, biology prediction, response, and prognosis | Diagnosis assistance, tumor biology prediction, response prediction, and recurrence/survival prediction | Research/translational stage | Internal AUC often fails to generalize; labels, cohorts, scanners, and protocols vary across institutions | TRIPOD + AI, CLAIM 2024, PROBAST + AI, external validation, prospective validation, transparent reporting, fairness checks, and decision-impact studies | [82-88] |
| AI-assisted segmentation/volumetric response tracking | Automated liver/tumor segmentation, volume tracking, new-lesion detection, and longitudinal response support | Workflow automation and quantitative response tracking | Selected workflow tools; broader response AI remains translational | Generalization drops across scanners, contrast protocols, and institutions; difficult failure-mode auditing | Segmentation reproducibility, multicenter prospective testing, human-AI workflow integration, reader-impact studies, and safety monitoring | [84,89-91] |
It is useful to separate three related but distinct concepts in post-treatment imaging: response measurement, response categorization, and decision impact. mRECIST is primarily a measurement framework. It recognizes that viable HCC is better reflected by arterial-phase enhancement than by the total treated mass, which may remain stable or even enlarge because of hemorrhage, necrosis, edema, or treatment cavity evolution. For this reason, mRECIST remains deeply embedded in HCC trials and routine locoregional therapy follow-up. Its strengths are familiarity, simplicity, and feasibility across multicenter studies. Its limitations are geometric and biologic: a one-dimensional measurement may underrepresent irregular, infiltrative, partially necrotic, multifocal, or heterogeneously treated tumors, and mRECIST does not fully capture extrahepatic progression or mixed intrahepatic responses unless paired with broader disease assessment[9].
qEASL and related three-dimensional enhancement-based approaches were developed to address this limitation by quantifying viable enhancing tumor volume rather than relying on a single enhancing diameter. This logic is particularly relevant after TACE, transarterial radioembolization (TARE), ablation, or combined locoregional therapy, where residual viable tumor may persist as nodular, crescentic, peripheral, or discontinuous enhancement within a complex treatment zone. qEASL is therefore best framed as a promising quantitative adjunct for selected response-assessment workflows, not as a universal replacement for mRECIST. Its main advantage is biological plausibility: it more directly represents the spatial burden of viable enhancing tumor. Its main barrier is implementation: segmentation, subtraction or registration quality, enhancement thresholds, phase timing, software platform, and local calibration all influence the final value[78].
LI-RADS treatment response assessment (TRA) provides a complementary solution at the reporting level. Unlike mRECIST or qEASL, LI-RADS TRA is not designed primarily to compute a continuous tumor burden; it standardizes how radiologists categorize treated observations as viable, nonviable, equivocal, nonevaluable, or nonprogressing according to treatment mechanism. The 2024 CT/MRI update is useful because it separates nonradiation and radiation-based treatment response patterns, while CEUS Nonradiation TRA extends structured real-time viability assessment to appropriate nonradiation therapies and resection follow-up. In practice, these frameworks are complementary: mRECIST remains the widely used trial and clinical response metric, qEASL provides a quantitative volumetric adjunct for complex residual enhancement, and LI-RADS TRA provides standardized language for multidisciplinary communication and management decisions[6,7].
Treatment response imaging in HCC is moving from diameter-only measurement toward mechanism-aware and volume-aware assessment, but these tools are not at the same stage of use. mRECIST is familiar and trial-ready; LI-RADS TRA provides a reporting language for post-locoregional therapy communication; qEASL remains a quantitative adjunct that still needs automated reproducible segmentation, harmonized thresholds, multicenter validation, and prospective decision-impact studies before broad implementation[6,7,9,78].
Taken together, mRECIST, qEASL, and LI-RADS TRA should be viewed as complementary rather than interchangeable tools. mRECIST remains the most familiar clinical and trial metric, qEASL provides a volumetric enhancement-based adjunct for complex residual viable tumor, and LI-RADS TRA provides standardized post-treatment reporting language for multidisciplinary communication[6,7,9,78].
COMPUTATIONAL IMAGING BIOMARKERS, RADIOMICS, AND AI
Radiomics and AI in HCC are better treated as task-specific tools than as a single technology class. For diagnosis, AI may support lesion detection, arterial-phase timing quality control, LI-RADS feature extraction, and risk stratification of indeterminate observations such as LI-RADS category 3 or 4. For tumor biology, models have been explored for microvascular invasion, histologic grade, cytokeratin 19 (CK19) or Ki-67 expression, molecular subtype, immune microenvironment, and recurrence risk. For treatment planning and follow-up, computational imaging may help estimate ablation margins, tumor territory, residual viable volume, new-lesion detection, and longitudinal response[79-84].
The most mature near-term application is likely workflow support rather than autonomous diagnosis. Automated or semi-automated liver and tumor segmentation can reduce measurement burden, improve volumetric consistency, and enable qEASL-like or volume-based response workflows. Longitudinal deep learning systems that combine segmentation, tumor volume tracking, and new-lesion detection illustrate how AI could eventually complement RECIST/mRECIST-style workflows. However, such systems should be framed as decision-support and measurement-assistance tools until external validation and clinical impact data show that they improve management decisions or patient outcomes[84].
The barriers to clinical translation are substantial. Many HCC radiomics studies remain retrospective, single-center, and small relative to the dimensionality of the feature space. Labels such as microvascular invasion, treatment response, recurrence, and progression-free survival are clinically meaningful but can be unstable across institutions because they depend on pathology sampling, treatment selection, follow-up interval, and competing risks. Imaging inputs are also heterogeneous: arterial timing, hepatobiliary phase quality, CT reconstruction kernel, MRI field strength, b-values, contrast agents, and scanner vendors can all shift radiomic features or deep learning representations. Segmentation is another major source of variability, particularly for infiltrative tumors, multifocal disease, necrotic regions, and post-treatment cavities[85].
For these reasons, the key question is no longer whether an HCC imaging AI model achieves a high internal area under the receiver operating characteristic curve (AUC), but whether it remains calibrated, reproducible, and clinically useful outside the development environment. Essential prerequisites include patient-level data splitting, prevention of data leakage, external multicenter validation, prospective or temporal validation, complete reporting of preprocessing and model selection, assessment of calibration and decision-curve net benefit, subgroup testing across etiology and scanner platforms, and evaluation of how the model changes decisions in a real multidisciplinary workflow. Phantom calibration and cross-vendor harmonization are especially important for quantitative biomarkers and radiomic features; explainability and failure-mode analysis are especially important for deep learning systems[85-88].
Methodological frameworks should be part of this translation pathway. The Image Biomarker Standardization Initiative (IBSI) provides a foundation for radiomic feature standardization. The Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis-Artificial Intelligence (TRIPOD + AI) statement supports transparent reporting of AI-based prediction models. The Checklist for Artificial Intelligence in Medical Imaging (CLAIM) 2024 is tailored to medical imaging AI reporting, and the Prediction model Risk Of Bias Assessment Tool-Artificial Intelligence (PROBAST + AI) helps evaluate risk of bias and applicability. These frameworks do not prove clinical utility by themselves, but they define the minimum level of transparency needed before HCC imaging AI can be compared across centers or considered for clinical deployment[85-88].
At present, radiomics and AI are more defensible as radiologist-supervised workflow tools than as autonomous diagnostic systems. They may help with HCC diagnosis assistance, tumor biology prediction, treatment response evaluation, recurrence prediction, and workflow automation, but most models remain at a research or translational stage. Their near-term value is likely to come from consistency, efficiency, and quantitative traceability inside established reporting workflows[84-91].
IMAGE-GUIDED INTERVENTION AND WHOLE-COURSE MANAGEMENT
The clinical value of imaging innovation is easiest to appreciate during intervention, where technical gains can be mapped directly to procedural success. Fusion ultrasound and electromagnetic tracking make it possible to target lesions that are inconspicuous on gray-scale ultrasound alone, thereby expanding candidacy for percutaneous ablation[30-32]. CEUS can then be reused immediately after ablation to assess residual perfusion and to direct same-session retreatment when needed[7].
For transarterial therapy, CBCT integrates preprocedural and intraprocedural information into a common coordinate system. Feeding-artery identification, tumor territory mapping, and confirmation of target coverage can all be improved within the angiography suite itself[47-50]. This is one reason HCC is an especially useful model for image-guided oncology: the same technological ecosystem that detects disease also helps deliver and verify therapy.
Response assessment closes the loop. mRECIST remains deeply embedded in trials and clinical practice, but structured CT/MRI and CEUS treatment response algorithms provide a more explicit language for classifying viable, equivocal, or nonviable disease after therapy[6,7,9]. As volumetric quantification becomes more practical, the next step will likely be better alignment between acquisition, segmentation, response criteria, and retreatment decisions, rather than wholesale replacement of existing frameworks.
CURRENT LIMITATIONS, STANDARDIZATION GAPS, AND TRANSLATIONAL BARRIERS
Seen from the pathway level, the remaining problem is less a lack of imaging tools than a lack of dependable translation across settings. Access is the first constraint. CEUS agents, spectral CT, 3 Tesla MRI, CBCT-equipped suites, PET/MRI, and new radiotracers are not distributed evenly across regions or reimbursement systems. A technology that works in a tertiary center will not improve HCC outcomes at population scale unless it can be placed into a realistic referral, reporting, and treatment workflow[2,3,66].
Technical variability is the second constraint. Iodine maps, diffusion metrics, stiffness measurements, and radiomic features all depend on acquisition, reconstruction, segmentation, and software choices. Deep learning reconstruction and new detector platforms can improve images, but they can also change texture, edge definition, or apparent enhancement. Thresholds developed on one scanner or protocol therefore require phantom calibration, cross-vendor harmonization, and transparent reporting before they are used as clinical decision rules[39,60,85].
Evidence maturity is the third constraint. CEUS, gadoxetic acid-enhanced MRI, MRE for selected risk questions, and CBCT-assisted transarterial therapy have enough clinical experience to guide current practice in appropriate settings[18,49,62]. Spectral CT has selected-use evidence but still needs broader threshold standardization. Photon-counting CT, FAPI-oriented molecular imaging, IVIM/DKI metrics, and many radiomics or deep learning models should remain labeled as translational until multicenter and prospective studies link them to patient management or outcomes[43,44,60,61,72,73,85-88].
Governance is the fourth constraint. AI prediction models are often reported with incomplete preprocessing, unclear label definitions, or only internal test performance. The TRIPOD + AI statement, CLAIM 2024, and PROBAST + AI now make these weaknesses easier to identify[86-88]. For HCC imaging, a credible translation pathway has to evaluate technical performance, clinical utility, workflow fit, and failure modes together.
FUTURE DIRECTIONS
The next useful advances will probably be those that connect one step of the pathway to the next. Ultrasound can remain the surveillance gateway if visualization scoring, CEUS problem solving, and fusion guidance are used to triage patients rather than to duplicate CT or MRI. CT progress should focus on calibrated spectral and photon-counting measurements for lesions and treated tumors, not only image appearance. MRI development should make hepatobiliary contrast, motion-robust dynamics, diffusion, elastography, and abbreviated protocols easier to deploy in patients who need repeated examinations. PET and hybrid imaging should be reserved for biologic or whole-body questions that CT and MRI cannot answer.
Across modalities, four priorities follow from this logic: multicenter protocol harmonization, prospective decision-impact studies, response frameworks that connect segmentation to retreatment decisions, and AI systems that improve consistency within existing standards. The aim is not to replace expert interpretation with one model or one modality. It is to make HCC imaging more comparable across centers, more explicit about uncertainty, and more useful at the point where management decisions are made[10].
This review addresses a specific problem in HCC imaging: how to judge whether a platform advance has moved far enough along the pathway to support clinical decisions. The synthesis separates established tools, selected or emerging uses, and translational technologies, and links them to surveillance, diagnosis, treatment planning, response assessment, and recurrence monitoring. That framing makes the maturity gap clearer. CEUS, gadoxetic acid-enhanced MRI, selected MRE, and CBCT-assisted therapy already support clinical care in defined settings, whereas spectral CT, photon-counting CT, FAPI PET, advanced diffusion metrics, radiomics, and many AI models still need standardization and decision-impact evidence. For the wider HCC field, the main contribution is a practical way to align technical development with clinical pathways. Better images matter, but reproducible measurements, common reporting language, and evidence that changes management will matter more for the next stage of HCC imaging.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the review: Xie Y, Cai J
Performed literature search and drafted the manuscript: Huang Y
Prepared the figures and tables: Huang Y
Critically revised the manuscript for important intellectual content: Xie Y, Cai J
All authors read and approved the final manuscript.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool ChatGPT (GPT-5.5, released 2026-04-23) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
Xie Y is the Guest Editor of the special issue entitled “New Imaging Perspectives for HCC in the Era of Personalized Medicine and Artificial Intelligence” in Hepatoma Research. Xie Y was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling and decision making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229-63.
2. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922-65.
3. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82:315-74.
4. Chernyak V, Fowler KJ, Kamaya A, et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology. 2018;289:816-30.
5. Kamaya A, Fetzer DT, Seow JH, et al. LI-RADS US surveillance version 2024 for surveillance of hepatocellular carcinoma: an update to the american college of radiology US LI-RADS. Radiology. 2024;313:e240169.
6. Aslam A, Chernyak V, Tang A, et al. CT/MRI LI-RADS 2024 update: treatment response assessment. Radiology. 2024;313:e232408.
7. Lyshchik A, Fetzer DT, Kono Y, et al. Liver Imaging Reporting and Data System contrast-enhanced US nonradiation treatment response assessment version 2024. Radiology. 2024;311:e232369.
8. Choi SH, Fowler KJ, Chernyak V, Sirlin CB. LI-RADS: current status and future directions. Korean J Radiol. 2024;25:1039-46.
9. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52-60.
10. Koo E, Singal AG. Hepatocellular carcinoma surveillance: evidence-based tailored approach. Surg Oncol Clin N Am. 2024;33:13-28.
11. Tzartzeva K, Obi J, Rich NE, et al. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: a meta-analysis. Gastroenterology. 2018;154:1706-18.e1.
12. Kudo M. Defect reperfusion imaging with sonazoid®: a breakthrough in hepatocellular carcinoma. Liver Cancer. 2016;5:1-7.
13. Aziz MU, Eisenbrey JR, Deganello A, et al. Microvascular flow imaging: a state-of-the-art review of clinical use and promise. Radiology. 2022;305:250-64.
14. Wilson A, Lim AKP. Microvascular imaging: new Doppler technology for assessing focal liver lesions. Is it useful? Clin Radiol. 2022;77:e807-20.
15. Jeon SK, Lee JY, Kang HJ, Han JK. Additional value of superb microvascular imaging of ultrasound examinations to evaluate focal liver lesions. Eur J Radiol. 2022;152:110332.
16. Dietrich CF, Nolsøe CP, Barr RG, et al. Guidelines and Good Clinical Practice Recommendations for contrast enhanced ultrasound (CEUS) in the liver - update 2020 - WFUMB in cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultraschall Med. 2020;41:562-85.
17. D’Onofrio M, Crosara S, De Robertis R, Canestrini S, Mucelli RP. Contrast-enhanced ultrasound of focal liver lesions. AJR Am J Roentgenol. 2015;205:W56-66.
18. Zhang Z, Ma C, Luo Y. Diagnostic value of liver contrast-enhanced ultrasound in early hepatocellular carcinoma: a systematic review and meta-analysis. J Gastrointest Oncol. 2023;14:626-35.
19. Liu Q, Liu T, Liu X, et al. The efficacy of modified contrast-enhanced ultrasound Liver Imaging Reporting and Data System (CEUS LI-RADS) using Sonazoid in diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Quant Imaging Med Surg. 2024;14:2927-37.
20. Makoyeva A, Kim TK, Jang HJ, Medellin A, Wilson SR. Use of CEUS LI-RADS for the accurate diagnosis of nodules in patients at risk for hepatocellular carcinoma: a validation study. Radiol Imaging Cancer. 2020;2:e190014.
21. Hawley J, Tang Y, Sjöström A, Fuentes-Alburo A, Tranquart F. The clinical utility of liver-specific ultrasound contrast agents during hepatocellular carcinoma imaging. Ultrasound Med Biol. 2025;51:415-27.
22. Luo Y, Huang Q, Wen D, Yan J, Liu F, Qiao L. Review of clinical applications of sonazoid ultrasound contrast for liver evaluation. Ultrasound Q. 2024;40:e00692.
23. Jeong WK, Kang HJ, Choi SH, et al. Diagnosing hepatocellular carcinoma using sonazoid contrast-enhanced ultrasonography: 2023 Guidelines From the Korean Society of Radiology and the Korean Society of Abdominal Radiology. Korean J Radiol. 2023;24:482-97.
24. Huang J, Gao L, Li J, et al. Head-to-head comparison of Sonazoid and SonoVue in the diagnosis of hepatocellular carcinoma for patients at high risk. Front Oncol. 2023;13:1140277.
25. Huang Z, Zhu RH, Li SS, Luo HC, Li KY. Diagnostic performance of Sonazoid-enhanced CEUS in identifying definitive hepatocellular carcinoma in cirrhotic patients according to KLCA-NCC 2022 and APASL 2017 guidelines. Insights Imaging. 2024;15:263.
26. Sandrin L, Fourquet B, Hasquenoph JM, et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29:1705-13.
27. Castera L, Forns X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48:835-47.
28. Xu C, Jiang D, Tan B, Shen C, Guo J. Preoperative diagnosis and prediction of microvascular invasion in hepatocellularcarcinoma by ultrasound elastography. BMC Med Imaging. 2022;22:88.
29. Zhong X, Long H, Chen L, et al. Stiffness on shear wave elastography as a potential microenvironment biomarker for predicting tumor recurrence in HBV-related hepatocellular carcinoma. Insights Imaging. 2023;14:147.
30. Ahn SJ, Lee JM, Lee DH, et al. Real-time US-CT/MR fusion imaging for percutaneous radiofrequency ablation of hepatocellular carcinoma. J Hepatol. 2017;66:347-54.
31. Lu YB, Huang YN, Weng YC, et al. Contrast-enhanced ultrasonography guidance avoids US-CT/MR fusion error for percutaneous radiofrequency ablation of hepatocellular carcinoma. BMC Med Imaging. 2024;24:323.
32. Jie T, Guoying F, Gang T, Zhengrong S, Maoping L. Efficacy and safety of fusion imaging in radiofrequency ablation of hepatocellular carcinoma compared to ultrasound: a meta-analysis. Front Surg. 2021;8:728098.
33. Flohr TG, Schaller S, Stierstorfer K, Bruder H, Ohnesorge BM, Schoepf UJ. Multi-detector row CT systems and image-reconstruction techniques. Radiology. 2005;235:756-73.
34. McCollough CH, Bruesewitz MR, Kofler JM Jr. CT dose reduction and dose management tools: overview of available options. Radiographics. 2006;26:503-12.
35. Coursey CA, Nelson RC, Boll DT, et al. Dual-energy multidetector CT: how does it work, what can it tell us, and when can we use it in abdominopelvic imaging? Radiographics 2010;30:1037-55.
36. Asmundo L, Rizzetto F, Srinivas Rao S, et al. Dual-energy CT applications on liver imaging: what radiologists and radiographers should know? A systematic review. Abdom Radiol. 2024;49:3811-23.
37. Bhayana R, Parakh A, Kambadakone A. Material decomposition with dual- and multi-energy computed tomography. MRS Communications. 2020;10:558-65.
38. Lv P, Lin XZ, Chen K, Gao J. Spectral CT in patients with small HCC: investigation of image quality and diagnostic accuracy. Eur Radiol. 2012;22:2117-24.
39. Reimer RP, Hokamp NG, Niehoff J, et al. Value of spectral detector computed tomography for the early assessment of technique efficacy after microwave ablation of hepatocellular carcinoma. PLoS One. 2021;16:e0252678.
40. Jensen CT, Gupta S, Saleh MM, et al. Reduced-dose deep learning reconstruction for abdominal CT of liver metastases. Radiology. 2022;303:90-8.
41. Jaruvongvanich V, Muangsomboon K, Teerasamit W, et al. Optimizing computed tomography image reconstruction for focal hepatic lesions: deep learning image reconstruction vs iterative reconstruction. Heliyon. 2024;10:e34847.
42. Caruso D, De Santis D, Del Gaudio A, et al. Low-dose liver CT: image quality and diagnostic accuracy of deep learning image reconstruction algorithm. Eur Radiol. 2024;34:2384-93.
43. Onishi H, Tsuboyama T, Nakamoto A, et al. Photon-counting CT: technical features and clinical impact on abdominal imaging. Abdom Radiol. 2024;49:4383-99.
44. Wildman-Tobriner B, Felice N, Kalisz KR, et al. Photon-counting CT effects on sensitivity for liver lesion detection: a reader study using virtual imaging. Radiology. 2025;314:e241568.
45. Kim SH, Kamaya A, Willmann JK. CT perfusion of the liver: principles and applications in oncology. Radiology. 2014;272:322-44.
46. Jiang T, Kambadakone A, Kulkarni NM, Zhu AX, Sahani DV. Monitoring response to antiangiogenic treatment and predicting outcomes in advanced hepatocellular carcinoma using image biomarkers, CT perfusion, tumor density, and tumor size (RECIST). Invest Radiol. 2012;47:11-7.
47. Wallace MJ, Murthy R, Kamat PP, et al. Impact of C-arm CT on hepatic arterial interventions for hepatic malignancies. J Vasc Interv Radiol. 2007;18:1500-7.
48. Tacher V, Radaelli A, Lin M, Geschwind JF. How I do it: Cone-beam CT during transarterial chemoembolization for liver cancer. Radiology. 2015;274:320-34.
49. Pung L, Ahmad M, Mueller K, et al. The role of cone-beam CT in transcatheter arterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017;28:334-41.
50. Kim DJ, Chul-Nam I, Park SE, et al. Added value of cone-beam computed tomography for detecting hepatocellular carcinomas and feeding arteries during transcatheter arterial chemoembolization focusing on radiation exposure. Medicina. 2023;59:1121.
51. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999;42:952-62.
52. Griswold MA, Jakob PM, Heidemann RM, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002;47:1202-10.
53. Rofsky NM, Lee VS, Laub G, et al. Abdominal MR imaging with a volumetric interpolated breath-hold examination. Radiology. 1999;212:876-84.
54. Maung ST, Tanpowpong N, Satja M, Treeprasertsuk S, Chaiteerakij R. MRI for hepatocellular carcinoma and the role of abbreviated MRI for surveillance of hepatocellular carcinoma. J Gastroenterol Hepatol. 2024;39:1969-81.
55. Huppertz A, Balzer T, Blakeborough A, et al. ; European EOB Study Group. Improved detection of focal liver lesions at MR imaging: multicenter comparison of gadoxetic acid-enhanced MR images with intraoperative findings. Radiology. 2004;230:266-75.
56. Golfieri R, Renzulli M, Lucidi V, Corcioni B, Trevisani F, Bolondi L. Contribution of the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI to dynamic MRI in the detection of hypovascular small (≤ 2 cm) HCC in cirrhosis. Eur Radiol. 2011;21:1233-42.
57. Liu X, Jiang H, Chen J, Zhou Y, Huang Z, Song B. Gadoxetic acid disodium-enhanced magnetic resonance imaging outperformed multidetector computed tomography in diagnosing small hepatocellular carcinoma: a meta-analysis. Liver Transpl. 2017;23:1505-18.
59. Woo S, Lee JM, Yoon JH, Joo I, Han JK, Choi BI. Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma: correlation with enhancement degree and histologic grade. Radiology. 2014;270:758-67.
60. Zhou Y, Zheng J, Yang C, et al. Application of intravoxel incoherent motion diffusion-weighted imaging in hepatocellular carcinoma. World J Gastroenterol. 2022;28:3334-45.
61. Wang WT, Yang L, Yang ZX, et al. Assessment of microvascular invasion of hepatocellular carcinoma with diffusion kurtosis imaging. Radiology. 2018;286:571-80.
62. Venkatesh SK, Yin M, Ehman RL. Magnetic resonance elastography of liver: technique, analysis, and clinical applications. J Magn Reson Imaging. 2013;37:544-55.
63. Lee DH, Lee JM, Yi NJ, et al. Hepatic stiffness measurement by using MR elastography: prognostic values after hepatic resection for hepatocellular carcinoma. Eur Radiol. 2017;27:1713-21.
64. Tamaki N, Higuchi M, Keitoku T, et al. Magnetic resonance elastography for the prediction of hepatocellular carcinoma in chronic hepatitis B. JGH Open. 2024;8:e13067.
65. Brunsing RL, Chen DH, Schlein A, et al. Gadoxetate-enhanced abbreviated MRI for hepatocellular carcinoma surveillance: preliminary experience. Radiol Imaging Cancer. 2019;1:e190010.
66. Maung ST, Deepan N, Decharatanachart P, Chaiteerakij R. Abbreviated MRI for hepatocellular carcinoma surveillance - a systematic review and meta-analysis. Acad Radiol. 2024;31:3142-56.
67. Yokoo T, Masaki N, Parikh ND, et al. Multicenter validation of abbreviated MRI for detecting early-stage hepatocellular carcinoma. Radiology. 2023;307:e220917.
68. Yao Y, Civelek AC, Li XF. The application of 18F-FDG PET/CT imaging for human hepatocellular carcinoma: a narrative review. Quant Imaging Med Surg. 2023;13:6268-79.
69. Park JW, Kim JH, Kim SK, et al. A prospective evaluation of 18F-FDG and 11C-acetate PET/CT for detection of primary and metastatic hepatocellular carcinoma. J Nucl Med. 2008;49:1912-21.
70. Mohebbi A, Kiani I, Mohammadzadeh S, Mohammadi A, Tavangar SM. Qualitative and quantitative differentiation efficiency of dual-tracer PET/CT with 18F-fluorodeoxyglucose and 11C-acetate for primary hepatocellular carcinoma: a systematic review and meta-analysis. Abdom Radiol. 2025;50:198-212.
71. Ghidaglia J, Golse N, Pascale A, Sebagh M, Besson FL. 18F-FDG /18F-choline dual-tracer PET behavior and tumor differentiation in hepatocellular carcinoma. A systematic review. Front Med. 2022;9:924824.
72. Zhang J, Jiang S, Li M, et al. Head-to-head comparison of 18F-FAPI and 18F-FDG PET/CT in staging and therapeutic management of hepatocellular carcinoma. Cancer Imaging. 2023;23:106.
73. Semeraro L, Frantellizzi V, Filippi L, Palumbo B, De Vincentis G, De Feo MS. Positron emission tomography with fibroblast activation protein-targeted radiopharmaceuticals in primary hepatic tumors: a systematic review. Appl Sci. 2025;15:2025.
74. Awali M, El Homsi M, Fraum TJ, et al. PET/MRI: pictorial review of hepatobiliary and pancreatic applications. Abdom Radiol. 2025;50:875-901.
75. Goertz RS, Bernatik T, Strobel D, Hahn EG, Haendl T. Software-based quantification of contrast-enhanced ultrasound in focal liver lesions--a feasibility study. Eur J Radiol. 2010;75:e22-6.
76. Tang A, Bashir MR, Corwin MT, et al. ; LI-RADS Evidence Working Group. Evidence supporting LI-RADS major features for CT- and MR imaging-based diagnosis of hepatocellular carcinoma: a systematic review. Radiology. 2018;286:29-48.
77. Lee S, Kim SS, Roh YH, Choi JY, Park MS, Kim MJ. Diagnostic performance of CT/MRI liver imaging reporting and data system v2017 for hepatocellular carcinoma: a systematic review and meta-analysis. Liver Int. 2020;40:1488-97.
78. Lin M, Pellerin O, Bhagat N, et al. Quantitative and volumetric European Association for the Study of the Liver and Response Evaluation Criteria in Solid Tumors measurements: feasibility of a semiautomated software method to assess tumor response after transcatheter arterial chemoembolization. J Vasc Interv Radiol. 2012;23:1629-37.
79. Lambin P, Rios-Velazquez E, Leijenaar R, et al. Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer. 2012;48:441-6.
80. Aerts HJ, Velazquez ER, Leijenaar RT, et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun. 2014;5:4006.
81. Gillies RJ, Kinahan PE, Hricak H. Radiomics: images are more than pictures, they are data. Radiology. 2016;278:563-77.
82. Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJWL. Artificial intelligence in radiology. Nat Rev Cancer. 2018;18:500-10.
83. Ahn JC, Qureshi TA, Singal AG, Li D, Yang JD. Deep learning in hepatocellular carcinoma: Current status and future perspectives. World J Hepatol. 2021;13:2039-51.
84. Xia Y, Zhou J, Xun X, et al. Deep learning for oncologic treatment outcomes and endpoints evaluation from CT scans in liver cancer. NPJ Precis Oncol. 2024;8:263.
85. Zwanenburg A, Vallières M, Abdalah MA, et al. The image biomarker standardization initiative: standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology. 2020;295:328-38.
86. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378.
87. Tejani AS, Klontzas ME, Gatti AA, et al. ; CLAIM 2024 Update Panel. Checklist for artificial intelligence in medical imaging (CLAIM): 2024 Update. Radiol Artif Intell. 2024;6:e240300.
88. Moons KGM, Damen JAA, Kaul T, et al. PROBAST+AI: an updated quality, risk of bias, and applicability assessment tool for prediction models using regression or artificial intelligence methods. BMJ. 2025;388:e082505.
89. Bilic P, Christ P, Li HB, et al. The liver tumor segmentation benchmark (LiTS). Med Image Anal. 2023;84:102680.
90. Gross M, Arora S, Huber S, Kücükkaya AS, Onofrey JA. LiverHccSeg: a publicly available multiphasic MRI dataset with liver and HCC tumor segmentations and inter-rater agreement analysis. Data Brief. 2023;51:109662.
91. Moawad AW, Morshid A, Khalaf AM, et al. Multimodality annotated hepatocellular carcinoma data set including pre- and post-TACE with imaging segmentation. Sci Data. 2023;10:33.
92. Tacher V, Lin M, Duran R, et al. Comparison of existing response criteria in patients with hepatocellular carcinoma treated with transarterial chemoembolization using a 3D quantitative approach. Radiology. 2016;278:275-84.
93. Xu J, Yin Y, Yang J, et al. Modified quantitative and volumetric response evaluation criteria for patients with hepatocellular carcinoma after transarterial chemoembolization. Front Oncol. 2023;13:957722.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.